Basic HTML Version


REVIEW
SA JOURNAL OF DIABETES & VASCULAR DISEASE
10
VOLUME 9 NUMBER 1 • MARCH 2012
Correspondence to: Dr Landi Lombard
Netcare Kuilsrivier Hospital, Cape Town
Tel: +27 0(21) 900-6350
e-mail: lclombard@mweb.co.za
S Afr J Diabetes Vasc Res
2012;
9
: 9–12
DPP-4 inhibitors (gliptins) in the management
of type 2 diabetes
LANDI LOMBARD
Introduction
Most readers of this journal will be aware of the huge pandemic
of non-communicable diseases, led by diabetes, particularly type 2.
This has been highlighted recently by theWorld Health Organisation
1
and was reported in our recent editorial.
2
Unlike the HIV pandemic,
where we are past the peak and are controlling and preventing
the disease, we have thus far been unsuccessful in making any
progress in the escalating diabetes pandemic. The peak is not in
sight, parallel to the massive increase in worldwide obesity.
Despite this increase, we as physicians are not faring well in
controlling diabetes. Worldwide, targets for managing diabetic
patients are not being met.
3,4
We therefore urgently need more
drugs in our armament to improve the control of diabetes, especially
in our own country.
As with the HIV pandemic, the scientific and pharmaceutical
industry has responded with many new drugs recently entering the
market and many to follow. One of these classes is the dipeptidyl
peptidase-4 inhibitors (DPP-4 inhibitors). Five of these molecules
have been developed (more are currently in development) and most
will probably be available in this country. To help clinicians make
decisions regarding these molecules, this review will briefly discuss
the molecules and assess their special features and differences.
Biochemistry and pharmacodynamics
DPP-4 inhibitors are GLP-1-based (glucagon-like peptide-1) therapy,
previously reviewed in this journal.
5
The DPP-4 inhibitors act by
inhibiting the serine protease DPP-4 enzyme responsible for the
rapid breakdown and short half-life of GLP-1.
6
The inhibition of
this enzyme prevents the metabolic clearance of the molecule and
therefore increases the insulinotropic activity of GLP-1.
It is well documented that diabetics have decreased GLP-1
production,
7
which to some extent limits the efficacy of the DPP-4
inhibitors. This limitation is because DPP-4 inhibitors can only prolong
the effect of the produced GLP-1 and not, as the GLP-1 analogues
do, increase or replace production to normal or supra-normal levels.
The increased levels of GLP-1 will have positive effects, including
blood glucose lowering, as summarised in Table 1.
5-9
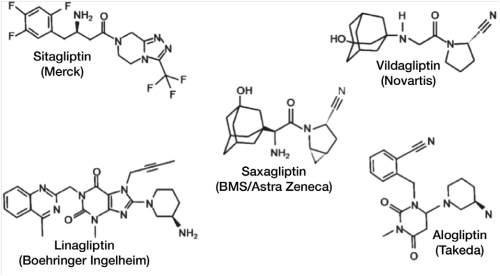
The DPP-4 inhibitors can be divided into two classes; those
which mimic the dipeptide structure (peptidomimetic) of the DPP-4
enzyme, and the so-called non-peptidomimetic class. Five molecules
will be discussed. The first three are vildagliptin,
10-12
sitagliptin
13-15
and saxagliptin
16,17
and all are peptidomimetics. The other two are
non-peptidomimetics called alogliptin
18,19
and linagliptin.
20,21
Their
structures can be seen in Fig. 1.
22
All five of these molecules are competitive, reversible inhibitors
of DPPs with a high affinity for DPP-4. Their modes of action differ
however. Sitagliptin,
1
alogliptin
18
and linagliptin
20
form non-covalent
bonds with the catalytic site. Vildagliptin
10
and saxagliptin
16
act by
a two-step process. A reversible covalent enzyme-inhibitor complex
is formed with a slow rate of inhibitor bonding and dissociation,
resulting in the enzyme slowly equilibrating between the active
and the inactive forms. This explains the much longer duration of
action of these drugs compared to their half-lives and this will have
implications for their pharmacokinetics.
Many studies have been published on the efficacy and potency
of each of these molecules, but only one compared them directly.
This study showed that there is very little difference in efficacy, but
that potency varied significantly, as measured by IC
50
.
23
There is a
marked variation in the half-life of the drugs, as can be seen in
Table 2.
12,15,17,24,25
The differences in half-life are reflected in the therapeutic doses
(ranging from 5 mg for saxagliptin to 100 mg for sitagliptin), and in
the dosing frequency (once daily for all, except vildagliptin which is
twice daily). Despite the differences in potency, when used at their
therapeutic doses, the effects of the inhibitors (extent of DPP-4
inhibition
in vivo
) are broadly similar. More than 90% inhibition is
achieved within 15 minutes of drug administration, with 70–90%
inhibition being sustained 24 hours post dose.
22
For vildagliptin, the
Table 1.
The effects of GLP-1.
5-9
1. Delay gastric emptying
2. Enhance satiety
3. Suppress appetite
4. Glucose-dependant improved insulin production by beta-cells
5. Suppress post-prandial glucagon release and hepatic glucose output
(glucose-dependent)
6. Improve beta-cell function and mass
7. Decrease beta-cell apoptosis (animal studies)
8. Enhance beta-cell neogenesis (animal studies)
Fig. 1.
The structure of the DPP-4 inhibitors.
22