

















 12 / 44
12 / 44

146
VOLUME 11 NUMBER 4 • NOVEMBER 2014
REVIEW
SA JOURNAL OF DIABETES & VASCULAR DISEASE
focus on achieving glycaemic targets but modifiable cardiovascular
risk factors such as hypertension, dyslipidaemia, kidney disease and
obesity must also be targeted.
10
There is currently a vast array of anti-diabetic drugs. Biguanides,
specifically metformin, is advocated as initial therapy, if not contra-
indicated and if tolerated.
11,12
Sulphonylureas remain popular,
despite weight gain, increased risk of hypoglycaemia and limited
long-term durability, because they are efficacious, affordable and
clinicians are familiar with them. Other classes include dipeptidyl
peptidase IV (DPPIV) inhibitors, glucagon-like peptide-1 analogues,
alpha-glucosidase inhibitors, meglitinides, thiazolidinediones, and
insulin. The pharmacological action and examples of the main
groups are shown in Table 1.
The newest addition to the armamentarium is the sodium
glucose co-transporter (SGLT) inhibitors and includes dapagliflozin,
canagliflozin, empagliflozin, ipragliflozin and tofoglilozin. None of
these drugs are currently registered in South Africa.
Sodium glucose co-transporters (SGLT) in healthy
individuals
There are various types of SGLTs, and these are listed in Table 2. This
section will focus on SGLT1 and SGLT2.
The kidney filters approximately 180 litres of plasma per day and
produces only one to two litres of urine. Therefore re-absorption of
sodium, water and other substances in the healthy non-diseased
kidney is substantial. This filtered fluid contains approximately 162 g
of glucose.
16
In non-diabetic individuals, 95%of the filtered glucose is
reabsorbed in the proximal convoluted tubules (PCT) of the nephron.
This is mediated by sodium glucose co-transporters (SGLT).
There are two subtypes of SGLT in the PCT of the nephron, SGLT
1 and SGLT 2. SGLT 2 is found in segment 1 and 2 of the PCT.
16,17
and is a high-capacity, low-affinity transporter responsible for 90%
of the re-absorption of glucose.
16,17
SGLT 1 is found in segment 3 of
the PCT and is a high-affinity, low-capacity transporter responsible
for re-absorption of 10% of filtered glucose.
16
SGLT 1 is also present
in the intestine and is responsible for absorption of glucose and
galactose.
16
SGLT in type 2 diabetes mellitus
The number and activity of SGLT receptors are increased in type 2
diabetes.
16,18
Therefore, although there is hyperglycaemia, the kidney
actually increases the re-absorption of glucose from the glomerular
ultra-filtrate, thus worsening the existing hyperglycaemia. The
reaction of the body to increase renal re-absorption seems counter-
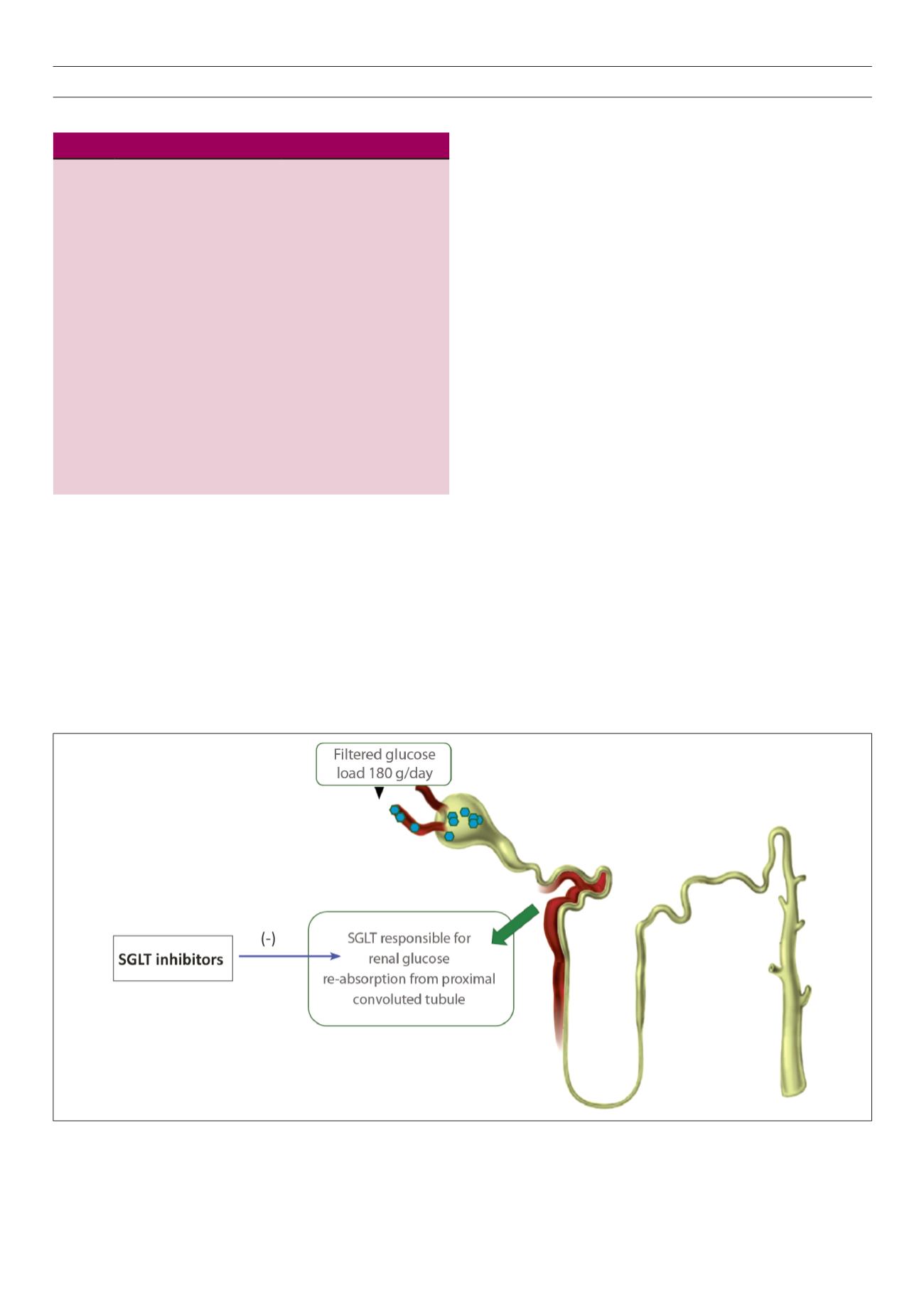
Fig. 1.
Sodium glucose co-transporter (SGLT) inhibitors reduce glucose re-absorption in the proximal tubule, leading to urinary glucose excretion and osmotic diuresis.
Modified from Ferrannini and Solini.
4
Table 2.
SGLT location and function
14,15
Location
Function
SGLT1 Small intestine, trachea,
kidney, heart and colon
Main uptake mechanism for
glucose and galactose in the
intestine; 10% of the renal
glucose re-absorption
SGLT2 Predominantly kidney. Small
amounts in cerebellum and
low levels in heart, salivary
gland, liver and thyroid
90% of the total renal
glucose re-absorption
SGLT3
Neurons of the small intestine
and in neuromuscular
junctions of skeletal muscle
Transports sodium upon
glucose binding
SGLT4
Intestine, kidney, liver, brain,
lung, trachea, uterus and
pancreas
Renal monosaccharide and/or
sodium re-absorption
SGLT5
Kidney
Possibly similar to SGLT2,
but role in monosaccharide
transport not established
SGLT6
Brain, spinal cord, kidney,
intestine
Monosaccharide transport