


















 15 / 48
15 / 48

SA JOURNAL OF DIABETES & VASCULAR DISEASE
REVIEW
VOLUME 12 NUMBER 1 • JULY 2015
13
guidelines regarding the assessment of first-, second-, and
third-line pharmacotherapy; the evidence underlying published
algorithms is biased in favour of peripheral neuropathic
pain disorders as opposed to central neuropathic pain; evidence
from trials is biased in favour of monotherapy over combination
therapy; guidelines and algorithms are sourced from appraisals
of independent heterogeneous controlled trials rather than head-
to-head comparative studies; there is a high number of negative
clinical trials with equivocal data; and the short duration of most
trials provides limited data on chronic neuropathic pain. Additionally,
the utility of current licensed drugs is further hindered by dose-
limiting side effects. Emerging evidence suggests the multifactorial
challenges associated with the treatment of neuropathic pain may
be surmountable by regenerative approaches based on the utility
of cell therapies.
Stem cells
Stem cells are undifferentiated cells capable of unlimited prolifera-
tion and self-renewal while retaining the potential towards
differentiation into any cell type of endodermal, ectodermal
or mesodermal origin. There are three main types of stem cells:
embryonic stem cells, adult stem cells, and induced pluripotent
stem cells.
The main advantages of stem cells hone in on their potential
use for regenerative therapies, with the overall aim of repairing or
replacing diseased tissues and organs. Stem cell technology provides
a potentially limitless purified population of patient- and disease-
specific cells, which confers a range of clinical benefits. These
include: understanding the pathogenesis of disease; facilitating
drug discovery; and generating cells for transplantation.
Embryonic stem (ES) cells
ES cells are pluripotent cells derived from the inner cell mass of
the developing blastocyst.
9
ES cells confer the advantage of being:
renewable; accessible to genetic modifications; and expandable
in vitro
for lengthy periods. Thus ES cells can be yielded in very
high purified quantities for potential regenerative purposes.
Disadvantages of ES cells include: a relatively high tumorigenic
potential; transplant rejection; and ethical concerns relating to
disaggregating the developing blastocyst.
10
Adult stem cells
Adult stem cells are multipotent undifferentiated cells. They are
derived from specific tissues within the embryo, foetus or adult e.g.
the SVZ situated throughout the lateral walls of the lateral ventricles,
which contains NSCs, or the bone marrow, which contains two
types of adult stem cells, namely, MSCs and haematopoietic
stem cells. The amniotic membrane is also a plentiful source of non-
immunogenic MSCs, which are easily and non-invasively harvested.
Amniotic membrane MSCs have demonstrable anti-inflammatory
properties, which have been used clinically in pain relief and wound
healing.
11,12
Advantages of adult stem cells include: self-renewability; fewer
ethical issues relative to ES cells; and the potential to be harvested
from easily accessible organs and expanded. Furthermore, adult
stem cells have a superior safety profile with a lower tumorigenic
potential relative to ES cells. Disadvantages include: a lower degree
of plasticity, expandability, and renewability, coupled with a greater
susceptibility to senescence compared to ES cells; and invasive
harvesting methods e.g. bone marrow trephine and biopsy to
obtain MSCs. Furthermore, in contrast to ES cells, adult stem cells
are rarer in number in mature tissues. This is significant as large
numbers of cells are needed for stem cell replacement therapies.
Induced pluripotent stem (iPS) cells
iPS cells are derived from non-pluripotent somatic cells such as
dermal fibroblasts, which have been transformed and genetically
‘reprogrammed’ into a pluripotent state akin to ES cells. This is
achieved by transfection with transcription factors such as Oct-3/4,
Sox 2 and Nanog, which are core transcription factors that repress
the expression profile of differentiated cells and activate an array
of genes involved in pluripotency.
13
Other key transcription factors
include Klf-4, Lin28 and c-Myc. Similarities to ES cells include: the
expression of certain stem cell genes and proteins; viable chimera
formation; chromatin methylation patterns; doubling times;
teratoma formation; embryoid body formation; and potency and
differentiability.
14
Four traditional strategies are available to reprogramme somatic
cells to an iPS cell state: viral transduction; nuclear transfer; cell
fusion; and cell explantation. Reprogramming is commonly achieved
with viral vectors, which can be either integrating e.g. retroviral or
lentiviral vectors, or non-integrating such as adenoviral vectors.
Limitations of the transcription factor approach to make iPS
cells include: a low throughput; mutations being inserted into
the target cell’s genome; tumours, especially with c-Myc; and
incomplete reprogramming. These limitations can be overcome by
novel techniques to make iPS cells, which include: ES cell-specific
miRNA to prompt iPS cell reprogramming;
15
using biomimicry with
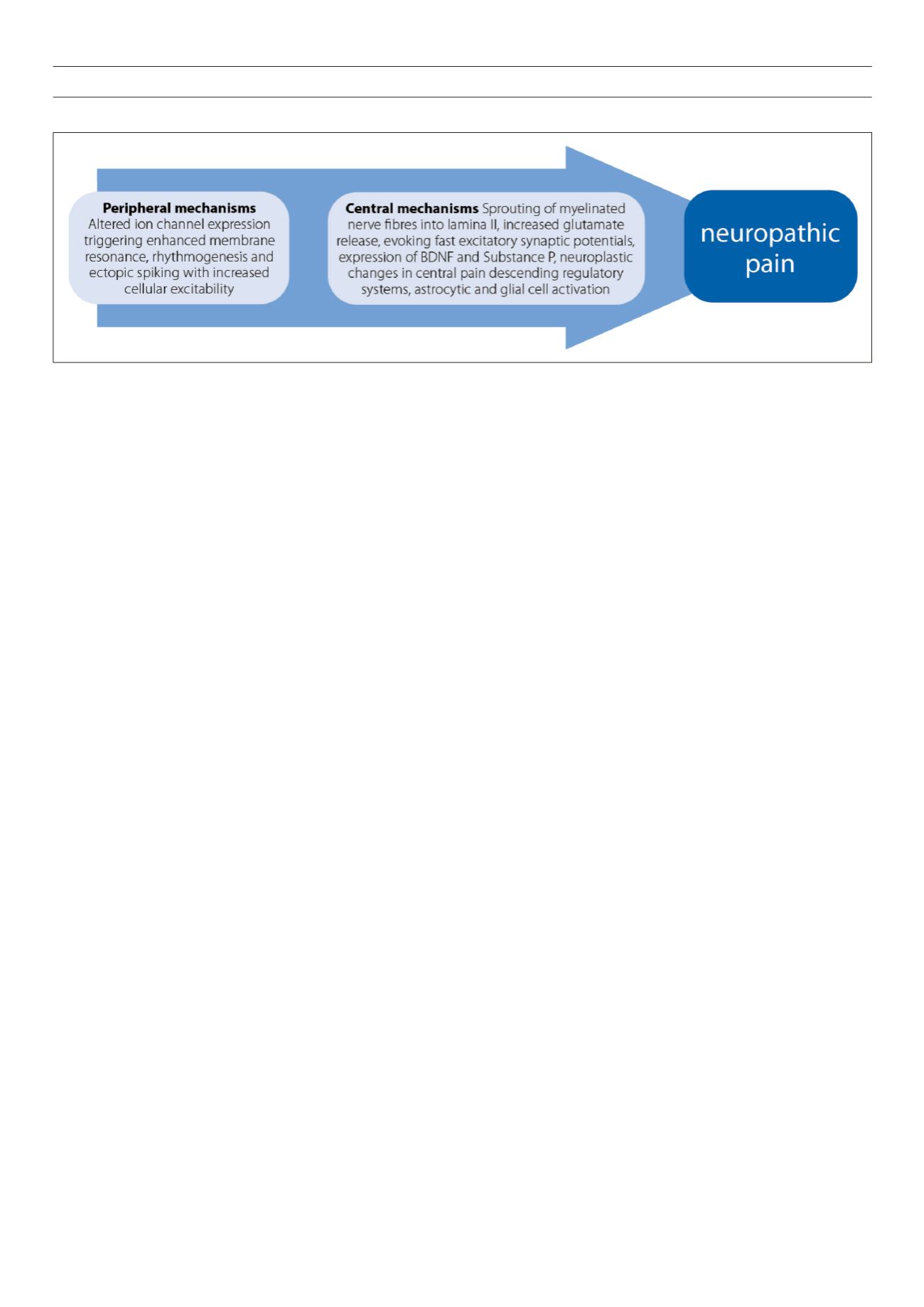
Fig. 1.
An overview summary of the peripheral and sensory mechanisms leading to neuropathic pain.