

















 7 / 44
7 / 44

SA JOURNAL OF DIABETES & VASCULAR DISEASE
RESEARCH ARTICLE
VOLUME 15 NUMBER 1 • JULY 2018
5
isolation media for gram-positive and -negative bacteria. The
wound specimens were inoculated on these media and incubated
appropriately at 35–37°C. All isolates were subjected to antibiotic
sensitivity testing using the disc diffusion technique.
The data generated were subjected to simple descriptive
statistical analysis using frequencies and percentages. Chi-squared
statistics was also employed where necessary. Statistical significance
was set at
p
< 0.05.
Results
Six-hundred and four individuals living with diabetes were admitted
within the three years this study lasted. There were 127 (21%)
diabetic patients living with foot ulcer(s). Eighteen (14.2%) had
incomplete records and were subsequently not included in the
analysis; 109 (85.8%) had complete results. All subjects had T2DM.
There were 44 females and 65 males (1:1.5) with a mean age of
53.5 ± 11.4 years. Other aspects of socio-demographic data are
depicted in Table 1.
Relevant clinical data in Table 2 show that the majority had had
DM for more than a decade, had had the foot ulcer for more than
six months and had poor glycaemic control on presentation. Most
patients admitted were in the age group 50–59 years, as depicted
in Table 3, while Table 4 shows the observed microbes and their
relative frequencies. Repeated swabs from three ulcers did not
grow any organism on bacterial culture. While one of these swabs
eventually became positive for fungi, two remained negative on
standard preparation for organisms, with very strict handling, and
for non-bacterial pathogens.
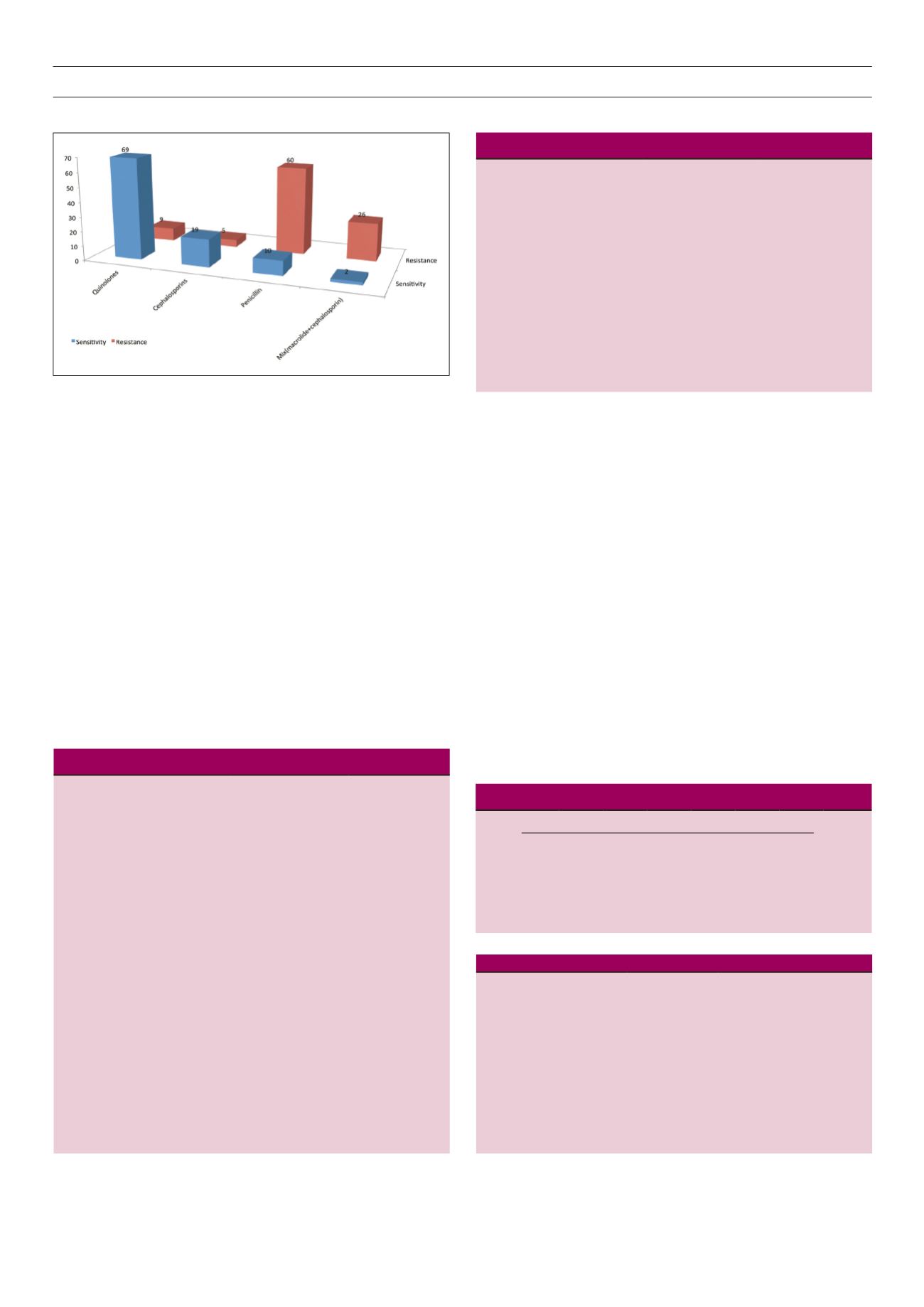
Fig. 1 is a graphical presentation of antibiotic sensitivity and
resistance pattern showing a high sensitivity to quinolones and
high resistance to penicillins.
Discussion
This was a retrospective study of adults living with T2DM who
presented with ulcers on the feet. They were mostly in the prime of
their lives, as evidenced by a mean age of 53.5 years. The zenith of
the impact of DM and its complications is thought to be highest in
individuals less than 60 years of age.
6,7
The majority of the patients
Table 1.
Socio-demographic characteristics of participants
Parameter
Frequency
Percentage
Age (years)
mean
range
distribution: 30–39
40–49
50–59
60–69
70–79
80–89
≥ 90
53.5 ± 11.4
38–92
3
17
38
28
15
7
1
2.8
15.6
34.8
25.7
13.8
6.4
0.9
Residence
Rural
Urban
49
60
44.9
55.1
Educational level
Primary
Secondary
Tertiary
65
30
14
59.7
27.5
12.8
Occupation
Farmers
Civil/public servant
Self employed
Unemployed (including retired)
58
34
5
12
53.2
31.2
4.6
11.0
Fig. 1.
Antibiotic sensitivity and resistance pattern.
Table 2.
clinical characteristics of participants
Parameter
Frequency
Percentage
DM duration (years)
< 5
5–10
≥ 11
24
33
52
22.0
30.3
47.7
Ulcer duration (months)
< 3
3–6
> 6
30
31
48
27.5
28.4
44.1
HbA
1c
at presentation
good (< 6.5)
poor (6.5– 8)
very poor (> 8)
24
35
50
22.0
32.1
45.9
Table 3.
Admission pattern in each age range
Age range (years)
Year 30–39 40–49 50–59 60–69 70–79 80–89 ≥ 90 Total
2012 1
4 12 11 3
2
0
33
2013 0
7 16 10 9
3
1
46
2014 2
6 10 7 3
2
0
30
Total
3
17 38 28 15
7
1
109
Table 4.
Implicated microbial organisms and their relative frequencies
Organism
Frequency
Percentage
Staphylococcus aureus
34
31.2
Escherichi coli
28
25.7
Pseudomonas
Streptococcus
20
12
18.4
11.0
Kliebsiella
8
7.3
Candida albican
1
0.9
Staphyloccoci + coliforms
4
3.7
No growth
2
1.8
Total
109
100.0