DRUG TRENDS
SA JOURNAL OF DIABETES & VASCULAR DISEASE
44
VOLUME 10 NUMBER 1 • MARCH 2013
occurred. This was despite the fact that more
than 80% of patients reached an HbA
1c
level
of less than 7%.
This lower rate of hypoglycaemia on
a gliclazide-based therapy may partially
be due to the fact that in experimental
animal studies, the newer sulphonylureas’
stimulatory action on insulin release is
related to glucose levels, with a lowered
stimulatory effect occurring on beta-cells of
the pancreas when glucose levels drop.
3
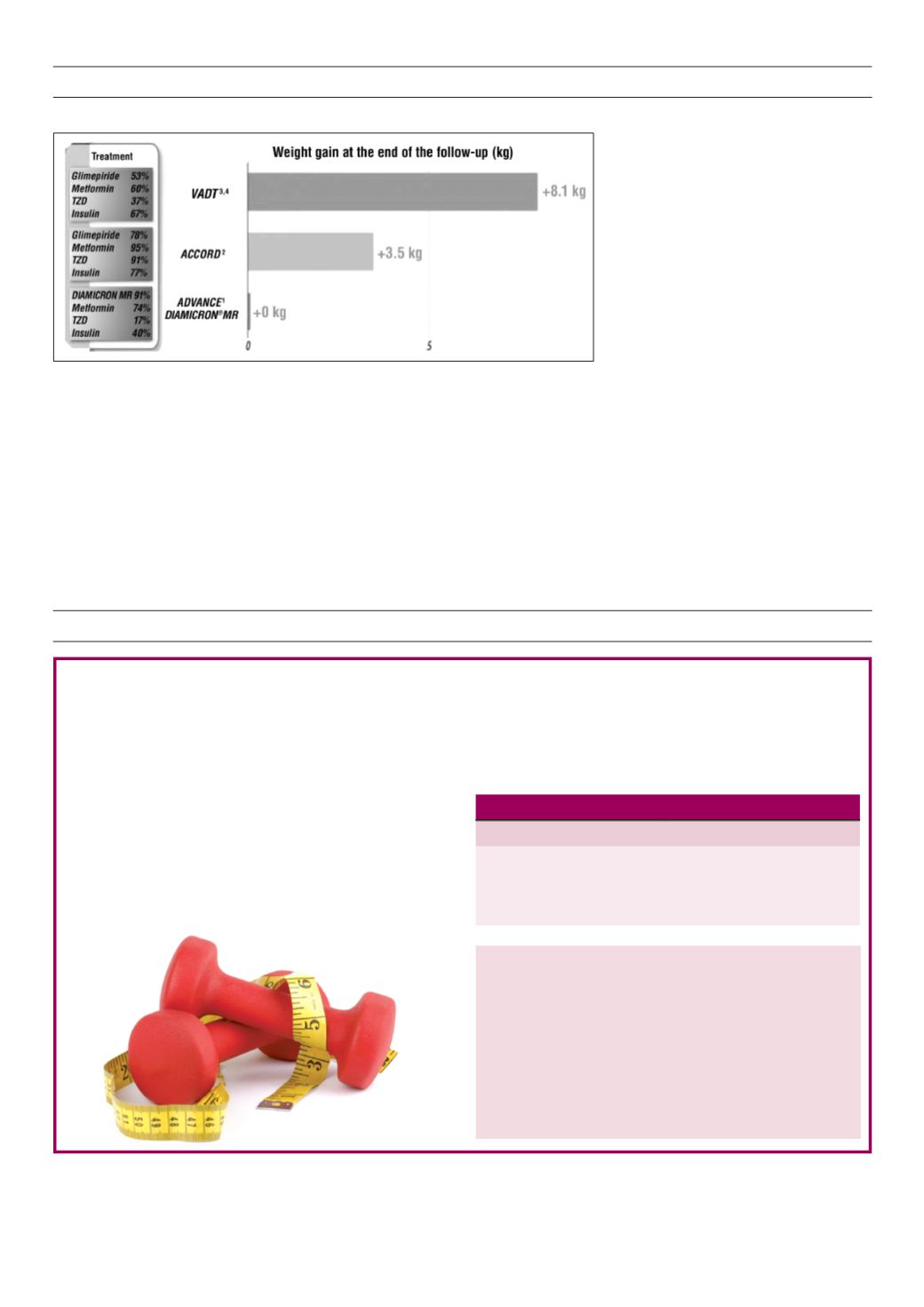
Weight gain and gliclazide MR use
In the ADVANCE trial there was no weight
gain seen in the patients with gliclazide MR
60 mg on intensive therapy, a very important
and relevant clinical observation (Fig. 2).
Renally impaired patients and gliclazide
In the ADVANCE trial, gliclazide MR 60 mg–
based therapy showed an overall renal-
protective effect and in the intensively
treated arm there was a 65% reduction in
Fig. 2.
Weight gain at the end of the follow-up peroid.
end-stage renal disease.
4
Currently, there is
no need to do renal function testing when
putting patients on gliclazide MR 60 mg
therapy.
With regard to patient compliance, the
availability of the Diamicron MR 60 mg
dose, which will halve the number of tablets
taken, will undoubtedly find favour with
patients and enhance overall compliance
and the clinical benefits that come along
with this.
References
1. The SEMDSA Guidelines 2012.
2. Patel A, MacMahon S
et al.
; the ADVANCE
collaborative group. Intensive blood glucose
control and vascular outcomes in patients with
type 2 diabetes.
N Engl J Med
2008;
358
: 2560–
2572.
3. Gregorio F, Ambrosi F, Cristallini S,
et al
. Therapeutic
concentrations of tolbutamide, glibenclamide,
gliclazide and gliquidone at different glucose
levels:
in vitro
effects on pancreatic
a
- and
β
-cell
function.
Diabetes Res Clin Pract
1992;
18
(3):
197–206.
4. Perkovic V,
et al
. Kidney international advance
online publication. 9 Jan 2013. Doi: 10.1038/
ki.2012.401.
Weight training lowers risk of type 2 diabetes
Risk reduction of type 2 diabetes with exercise
Exercise type
Risk reduction in type 2 diabetes
> 150 min/week weight training 34% (95% CI: 7–54%)
> 150 min/week aerobic training 52% (95% CI: 45–58%)
> 150 min/week combined training 59% (95% CI: 39–73%)
SAJDVD recommended action
For patients unwilling or unable to perform aerobic exercise,
weight training may be valuable in reducing the risk of
developing type 2 diabetes. Adding weight training to aerobic
exercise appears to give further protection and should be
encouraged in all at-risk patients.
Reference
1.
Grøntved A, Rimm E, Willett W,
et al
. A prospective study of weight training
and risk of type 2 diabetes mellitus in men.
Arch Intern Med
Published
online August 6, 2012. doi:10.1001/archinternmed.2012.3138.
M
en involved in weight training for more than 150 minutes
a week have a 34% lower risk of type 2 diabetes than
those doing no exercise. Although regular physical exercise is the
cornerstone of diabetes prevention and management, the role of
weight training has not been previously studied in detail.
The on-going prospective Health Professionals Follow-up study
evaluates the risk of developing diabetes in 32 000 healthcare
professionals aged 40–75 years.
1
For each 60 minutes of weight
training per week, the risk decreased by 13% (95% CI, 6–19%,
p
< 0.001).
The study also confirmed that men doing aerobic exercise for
more than 150 minutes a week had a 52% lower risk of type 2
diabetes than those doing no exercise. However, the combination
of the two forms of exercise was associated with an even greater
benefit, with a 59% reduction in type 2 diabetes risk in those
engaged in both aerobic exercise and weight training for more
than 150 minutes per week.
EVIDENCE IN PRACTICE


