SA JOURNAL OF DIABETES & VASCULAR DISEASE
DRUG TRENDS
VOLUME 7 NUMBER 3 • SEPTEMBER 2010
131
Drug Trends
Novo Nordisk update meeting at CDE
The weight of diabetes: South African opinion leaders set a new clinical framework
Looking at weight gain and how to get
patients to lose weight in a NEW context was
the theme of the Novo Nordisk/Life Scan-spon-
sored forum at the CDE meeting in Johannes-
burg last month.
New perspectives
• Type 1 and type 2 diabetes are the same
disorder of insulin resistance, set against a
different genetic background.
• Being overweight accelerates the tempo of
β
-cell loss, so the phenotype of type 1 and
type 2 diabetics converges over time.
• Post-prandial dysglycaemia upregulates the
β
-cell, driving it to failure.
• Doctors have an ethical responsibility to
tell their patients that type 2 diabetes is
a potentially curable disease. Intensive
lifestyle change and bariatric surgery can
achieve a more than 80% cure rate.
• Sibutramine is still an effective weight-loss
drug when used in appropriate patients,
essentially those without cardiovascular dis-
ease.
• ‘Testing’ is the secret to diabetes care in
both type 1 and type 2 diabetes. The cli-
nician must educate the patient to under-
stand the individual disease pattern (three
days of six tests daily from breakfast to
bed), and then address the pattern with the
patient to set suitable parameters of glu-
cose control.
• Modern man’s limbic system of emotional
attachment to attractive, flavourful food
overrides the satiety centre.
• Health professionals should lead by example
and there should be weight audits of both
patients and staff in diabetes practices.
The weight of the world
Prof P Joshi, Diabetes Care Centre, Pretoria
Weight loss is vital to reducing diabetic morbid-
ity and deaths. In diabetic patients, a decrease
in weight of 5 kg or more reduces the risk of
death by 50%; just as an increase in weight
(6–7 kg) increases the risk of death by 50%.
1
Health professionals must lead by example,
particularly in Africa where obesity is driving the
diabetic explosion. In fact, worldwide, death
from diabetes in 2007 has equalled the HIV-
related death of 2002 when antiretrovirals were
not readily available in developing countries.
Prof Joshi appealed to CDE units to intro-
duce a weight audit in their practices – for
both patients and staff. ‘We need to be advo-
cates of social change in South Africa with
regard to our food and lifestyle choices’, Prof
Joshi concluded.
Understanding the mechanisms of
weight gain
Dr Fraser Pirie, University of KwaZulu-Natal
The reasons for developing obesity are com-
plex and interrelated:
• a vulnerable genetic profile and environ-
mental influences of lifestyle and nutrition
• control by the ‘upper-order’ hypothalamus,
cortex and limbic system
• the presence of gastrointestinal tract
microbes and peptides
• nutrition in early life
• factors/hormones that regulate appetite
and are anorexigenic.
Dr Pirie predicts that there will be a flood of
new data on the genetic front with regard to
obesity in the next decade, which will continue
to influence clinical practice. A recent review
is of considerable value in understanding this
arena.
2
In the interim, clinicians must recognise the
therapeutic aspects of weight gain in type 2
diabetes and seek to use agents with the least
weight gain (Table 1). Dr Pirie pointed out
that metformin does limit weight gain when
patients are put on insulin; 50% of weight
gain occurs in the first three months of insu-
lin therapy, thereafter it slows. Insulin detemir
causes less weight gain due to its lipophylic
nature, slow release, less hypoglycaemia and
central anorexigenic effect.
3
In the LOOK AHEAD long-term study of
type 2 diabetic patients, increased physical
activity showed the strongest correlation with
weight loss,
4
while orlistat contributed little to
weight loss.
Weight gain in the younger
population
Dr Dave Segal, paediatric endocrinologist,
University of the Witwatersrand
Dr Segal sketched the neuro-economics of food
intake, particularly for children where food
procurement requires no energy expenditure –
a walk to the fridge or the school tuckshop!
Children are consuming huge amounts of
fructose, which is increasingly being used as
a natural sweetener in a syrup format. ‘Excess
fructose goes directly to fat’, he noted.
Ascribing the worldwide increase in type 1
and type 2 diabetes primarily to weight gain,
which correlates with the risk of developing
pancreatic islet cell auto-immunity in children
with a first-degree relative with type 1 diabe-
tes,
5
Dr Segal urged South African practition-
ers to place more emphasis on the need for
weight loss in younger diabetic patients.
Type 2 diabetes is a potentially
curable disease
Dr Greg Hough, specialist endocrinologist,
East London
Dr Hough pointed out that type 2 diabetes can
be cured by sufficient weight loss and bariatric
(gastric bypass) surgery, which results in a 80
to 87% cure rate. ‘The risks of bariatric surgery
are the normal risks of surgery, with very few
additional risks following treatment, although
patients are advised to adopt a moderate-fat
diet to avoid the risk of gallstones.’
Pointing out that exercise is vital to the
maintenance of weight loss, Dr Hough cited
the SCOUT study of sibutramine, which
showed that it is still an effective drug and one
of the few to induce significant weight loss
when used in appropriate patients.
‘Clearly sibutramine should be avoided in
patients with cardiovascular disease and in
those on MAOI, erythromycin and ketocona-
zole, which interfere with the P450 system.
Exenatide use results in a bit more impressive
weight loss with patients losing on average 4.5
kg over an 18-month period.’
J Aalbers, Special Assignments Editor
1. Daniels SR.
Future Child
2006;
16
(1): 47–67.
2. Fawcett KA, Barroso I.
Trends Genet
2010;
26
(6):
266–274.
3. HallischmidM,
etal
.
Diabetes
2010;
59
(4):1101–1107.
4. Wadden T,
et al
.
Obesity
2009;
17
(4): 713–722.
5. Couper JJ,
et al
.
Diabetes Care
2009;
32
(1): 94–99.
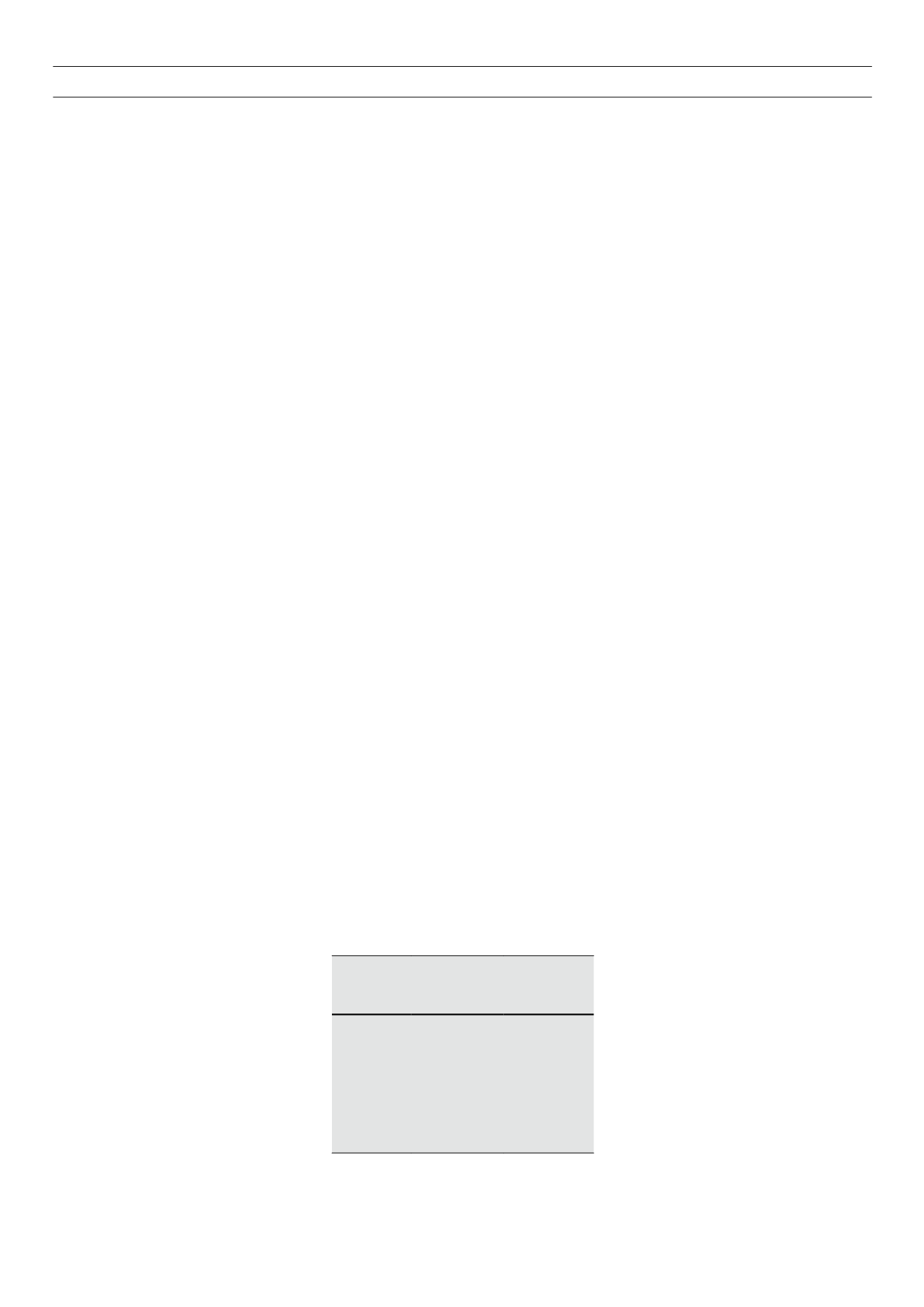
Table 1.
Effect of therapy for type 2 diabetes
on weight
Weight loss Weight neutral Weight gain
Pramlintide Metformin
Sulphonylureas
(least with
gliclazide MR)
GLP-1 agonist Acarbose
Glinides
DPP4-inhibitors TZD (thiazolidin-
ediones) Insulins


