


















 8 / 48
8 / 48

6
VOLUME 12 NUMBER 1 • JULY 2015
REVIEW
SA JOURNAL OF DIABETES & VASCULAR DISEASE
the emphasis on selection of drug therapy via statins has shifted to
the blood level of low-density lipoprotein (LDL) cholesterol.
16
In South Africa in 2000, high blood cholesterol levels have been
estimated to have caused 24 144 deaths (95% CI: 22 404–25
286) or 4.6% of all deaths.
17
Studies in the Cape Peninsula and
in the South African Indian population support links between lipid
abnormalities and coronary heart diseases.
18,19
Severely obese South
African white women have greatly reduced values for serum high-
density lipoprotein (HDL) cholesterol or ‘good’ cholesterol, rather
than high levels of LDL cholesterol.
20
Lipids in diabetes: the role of statins
The ideal approach to nip diabetes in the bud is by testing HbA
1c
values in those with the metabolic syndrome or obesity, and then
to go for weight loss induced by combined diet and exercise. In
those with established type 2 diabetes (DM2), a population study in
Hong Kong suggested that statin therapy attenuated the associated
increased cancer risk.
21
For diabetes, in a large study with 215 725
person-years of follow up, statin use before the diagnosis of diabetes
reduced diabetic retinopathy (hazard ratio 0.60, 95% CI: 0.54–0.66;
p
< 0.0001), diabetic neuropathy (HR 0.66, 95% CI: 0.57–0.75;
p
< 0·0001), and gangrene of the foot (HR 0·88, 95% CI: 0.80–0.97;
p
= 0.010).
22
Regarding the general adult population, statins are
recommended as first-line therapy in those up to and including 75
years of age, who have clinical atherosclerotic cardiovascular disease
(ASCVD) (Table 4 in Stone
et al
.
23
).
Exercise versus drugs
In studies on the secondary prevention of coronary heart disease and
pre-diabetes, randomised trials on exercise interventions suggest
that exercise and many drug interventions are often potentially
similar in terms of their mortality benefits, rehabilitation after
stroke, treatment of heart failure, and prevention of diabetes.
24
This
important observation reinforces the essential role of exercise in
any programme aimed at overall cardiovascular health (Table 1).
Banting first linked diet to mortality
Banting in his pamphlet
25
in 1869 emphasised the role of diet in
weight loss, stating that: ‘The dietary is the principle point in the
treatment of corpulence.’ The key points in the Banting diet were
his method of reducing obesity by avoiding fat, starch and sugar
in the food. Therefore the proposal that the Banting diet is similar
to the Noakes high-fat diet
3
appears to need re-appraisal. Banting
also made wider overall claims that the diet was ‘a simple remedy
to reduce and destroy superfluous fat; it may alleviate if not cure
gout; prevent or eradicate carbuncles, boils, dyspepsia, makes life
more enjoyable, and promotes longevity’. One interesting small but
important point is that Banting took the fat off the gravy. For these
reasons, it seems preferable to separate the Banting diet from the
Noakes low-carbohydrate, high-fat diet.
Israeli study and new Atkins diet
The low-carbohydrate, high-fat diets that were introduced by
Atkins and his successors
26
have had very wide influence. Some of
the key features are as follows, with the relevant book pages given
in brackets:
• Protein intake though high has recommend protein ranges (51).
• Fat intake though also high, has a desirable range (70).
• Vegetables including avocadoes are the basis of the permitted
carbohydrate intake (102).
In a major landmark Israeli diet, the new Atkins diet was compared
with others from the same Israeli population group in a dedicated
communal restaurant where the food intake could be monitored.
27
In the group given the new Atkins diet, besides weight loss, the
blood cholesterol pattern showed some favourable changes.
In the comparative group taking a calorie-limited Mediterranean
diet, similar changes were found in weight loss and blood lipid
levels. However, the Mediterranean diet was calorie limited whereas
the Atkins group had a spontaneous loss of appetite. The molecular
mechanism to explain the appetite loss is not clear. Reservations are
that there was no placebo group and the study was too short to
judge any clinical effects on cardiovascular events.
A broadly similar conclusion was reached in a meta-analysis
of diets of varying carbohydrate and lipid composition, the new
Atkins diet is one of several reduced-calorie diets that have all
resulted in clinically meaningful weight loss, regardless of which
macronutrients they emphasised.
28
What about high-fat weight-losing diets?
The two potential problems with high-fat diets lie in their adverse
effects on the blood lipoprotein pattern, and on the impairment
of specific mental functions, as observed by Kieran Clarke in
Oxford students. In the Oxford study, a short-term, high-fat, low-
carbohydrate diet led to higher circulating free fatty acid (FFA)
concentrations, impaired patterns of myocardial high-energy
phosphate metabolism, and decreased cognition in healthy
subjects.
29
The site of these deleterious effects on the brain was the
hippocampus. In the heart, sophisticated non-invasive nuclear
imaging techniques measured levels of high-energy phosphate
compounds, which were relatively low in those taking the high-
fat diet. The proposal was that elevated circulating FFA levels were
underlying the cognitive and cardiac abnormalities. Therefore
Clarke and her associates conclude that high-fat, low-carbohydrate
diets are potentially detrimental to human heart and brain.
29,30
For these reasons, there are arguments to support the view that
the diet overweight persons could best start is with a new Akins
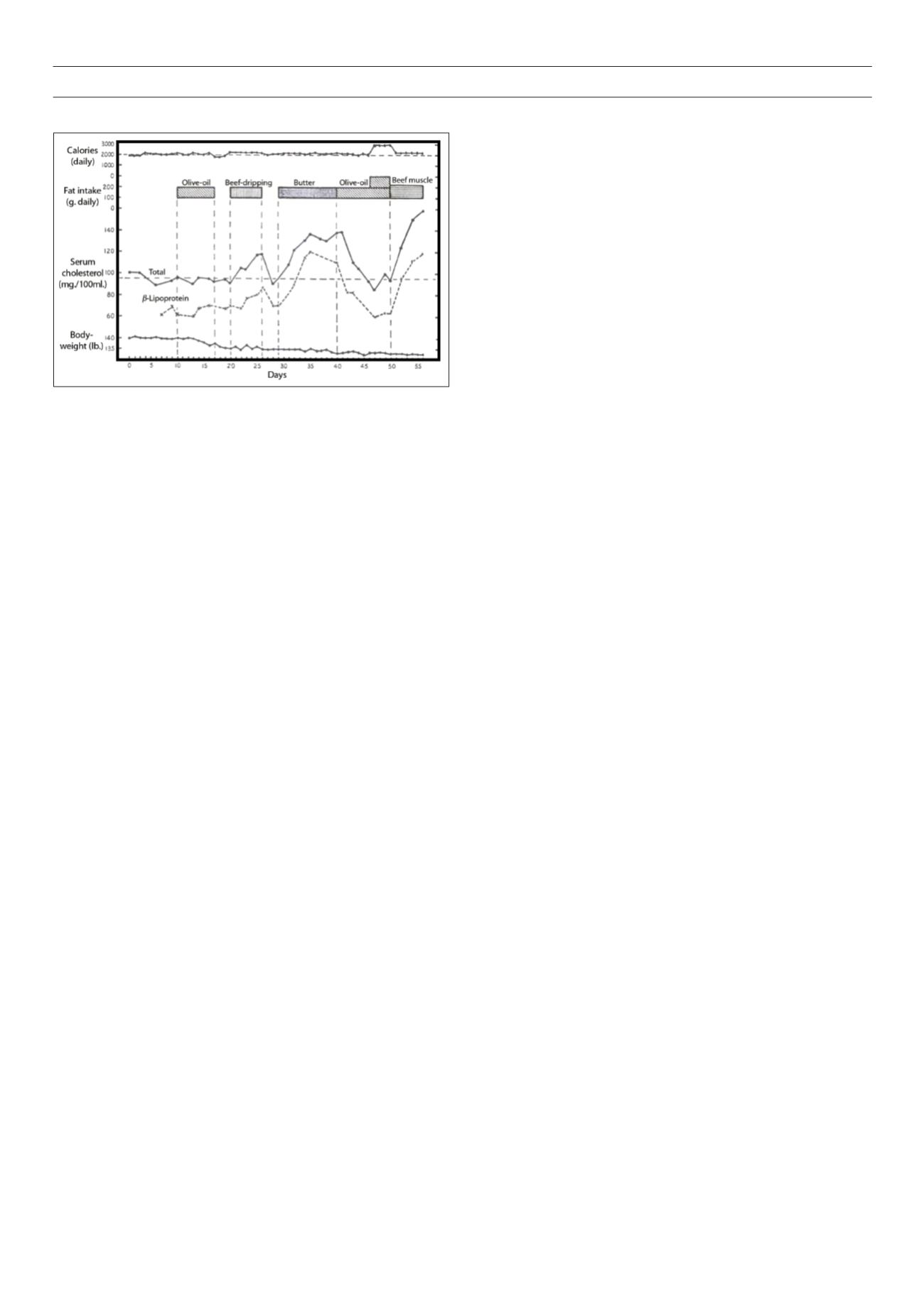
Fig 1.
A historical study in Cape Town. The effect of dietary fats on blood lipid
levels and their relation to ischaemic heart disease, neutralised by the effect of
added olive oil. Note the rapid rise in serum cholesterol levels with the provision
of the high-butter diet. All values were obtained in the Metabolic Unit, University
of Cape Town, South Africa. From Bronte-Stewart.
14