

















 8 / 42
8 / 42

RESEARCH ARTICLE
SA JOURNAL OF DIABETES & VASCULAR DISEASE
6
VOLUME 17 NUMBER 1 • JULY 2020
adjust for possible simultaneous confounding of the risk factors, a
multivariate logistic regression was fitted.
The stepwise model selection method was employed to come
up with the final model, which included the following risk factors:
type of hospital, age, parity, MUAC and history of macrosomia for
the WHO criteria. Similarly, a multivariate linear regression was
used to assess the relationship between RBG and the risk factors.
The final selected model included hospital type, BMI and history of
macrosomia.
SAS software version 9.3 (SAS Institute, North Carolina State
University) was used for analysis and all inferences were made at
the 0.05 significance level.
Results
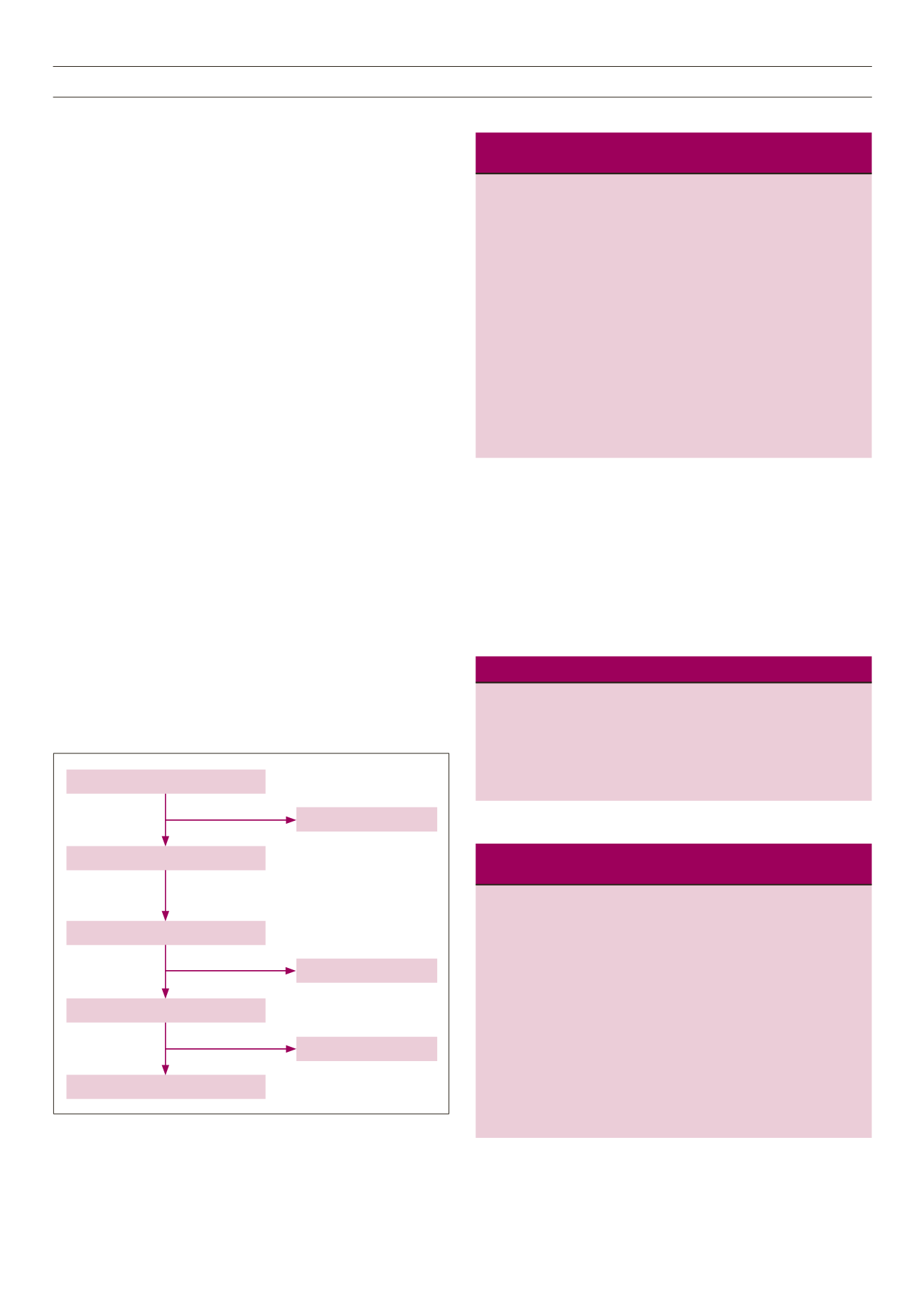
All participants were recruited from urban Blantyre. Fig. 1 shows a
flow chart of participants recruited in the study.
The study population was predominantly young with an average
age of 25.8 years (25th, 50th and 75th percentiles: 22, 25 and 30,
respectively). Six per cent of the women were above 35 years of
age, 66.4% were in the third trimester and 24% were between 24
and 28 weeks’ gestational age. Table 1 compares the demographic
characteristics of women in government and private ANCs.
Women at government-funded facilities were younger, of
higher parity and gravidity, had a lower pregnancy BMI and were
more likely to be HIV positive. Based on MUAC, 9% of the women
were overweight (MUAC 28–31 cm) and 1% were obese (MUAC
≥ 32 cm). There was no difference in the average MUAC between
government and private ANCs. When the BMI in pregnancy was
calculated, half of the women had a normal BMI (average BMI
26 kg/m
2
; 50th percentile 25).
Three per cent of the women had hypertension, but this was
not explored further to determine whether this was pre-eclampsia
or pre-existing hypertension. Eleven per cent of the women had
HIV and of these, 61% had documented records of being on anti-
retroviral therapy.
Tables 2 and 3 show RBG and OGTT results. Only three women
(0.1%) had an RBG level above 11.1 mmol/l. Twelve women (0.5%)
were hypoglycaemic. There was a significant association between
RBG level and attending government ANCs and BMI.
Based on the OGTTs, the overall prevalence of GDM was
1.6% (
n
= 5) and 24.8% (
n
= 65) by WHO and IADPSG criteria,
respectively. The simple kappa coefficient was calculated to
Table 1.
Comparison of demographic characteristics between govern-
ment and private ANCs
Government ANCs Private ANCs
Characteristics
(
n
= 2044)
(
n
= 178)
p
-value
Age (years), mean ± SD 25.8 ± 0.25
29.4 ± 0.6
< 0.0001
Gestational age (weeks),
26.9 ± 0.36
27.6 ± 3.2
0.68
mean ± SD
Parity, mean ± SD
1.2 ± 0.05
0.76 ± 0.13 < 0.0001
Gravidity, mean ± SD
2.5 ± 0.05
2 ± 0.12 < 0.0001
BMI in pregnancy,
26.2 ± 0.3
27.7 ± 0.8
0.0003
mean ± SD
MUAC (cm), mean ± SD 23.7 ± 0.15
23.5 ± 0.6
0.3646
Hypertension,
n
(%)
97 (4.7)
6 (3.3)
0.6574
HIV,
n
(%)
205 (10.0)
15 (8.4)
0.01
DM family history,
n
(%)
15 (0.7)
43 (24.1)
0.1573
Previous miscarriage,
n
(%)
361 (17.6)
41 (23.0)
0.308
ANC, antenatal clinic; BMI, body mass index; MUAC, mid upper-arm
circumference; DM, diabetes mellitus.
Table 2.
Risk factors associated with increasing RBG levels
Parameter
Standard
Variable
estimate
error
t
-value
p
-value
Government ANC –15.50589 4.763
–3.26
0.0013
BMI
1.09278 0.37628
2.90
0.0041
Macrosomia
–22.14294 12.98251 –1.71
0.0898
RBG, random blood glucose; ANC, antenatal clinic; BMI, body mass index.
Table 3.
Comparison of RBG and fasting glucose levels and GDM
prevalence by OGTTs in government and private ANCs
Government
Private
Variable
ANCs
ANCs
Overall
OR (95% CI)
RBG (g/dl),
94.4 ± 20 107 ± 24 94 ± 21
mean ± SD
Fasting glucose
84 ± 16
70 ± 16 81 ± 19
(g/dl), mean ± SD
2-h glucose (g/dl), 84 ± 18
86 ± 53 84 ± 17
mean ± SD
GDM (WHO),
1.4 (0.04–5.5)
0.04 (0–1) 1.6 (0.3–4) 3.5 (0.08–8.1)*
% (95% CI)
GDM (IADPSG), 31.7 (24.6–39.8) 7.8 (3–19.1) 24.8 (19–32) 5.5 (1.9–16)*
% (95% CI)
*GDM prevalence odds ratio for government ANCs vs private ANCs.
RBG, random blood glucose; ANC, antenatal clinic; GDM, gestational
diabetes mellitus; OGTT, oral glucose tolerance test.
Fig. 1.
Recruitment of participants. RBG, random blood glucose; OGTT, oral
glucose tolerance test.
2 350 ANC asked for consent
2 274 consented for RBG
2 222 included in RBG analysis
250 randomly selected for OGTT
193 included in OGTT analysis
76 declined
52 incomplete results
57 absent for OGTT