REVIEW
SA JOURNAL OF DIABETES & VASCULAR DISEASE
6
VOLUME 11 NUMBER 1 • MARCH 2014
allow behavioural adaptation in people with type 1 diabetes.
Psychomotor function is important for simple day-to-day tasks
such as tying shoe laces or preparing a meal, and any occupational
activity that requires precise motor movements. Spatial ability, which
allows humans to deal with two- and three-dimensional objects
and navigation, deteriorates significantly during hypoglycaemia in
people with type 1 diabetes.
19
Mood, emotion and motivation
Mood is often assessed in two basic domains,
20
namely tense
arousal (feeling anxious or nervous rather than relaxed or calm)
and energetic arousal (feeling lively and active rather than tired
and sluggish). Hedonistic tone (happiness versus sadness) can also
be evaluated.
21
Hypoglycaemia provokes negative emotions. Tense
arousal is increased and energetic arousal is reduced, producing a
state of ‘tense tiredness’, a combination that is rarely observed in
response to any other type of stress.
22-24
Hedonistic tone declined
in non-diabetic healthcare professionals during experimental
hypoglycaemia, who on questioning expressed a much more
pessimistic view of their career prospects.
24
Feelings of anger also
increase in some people during hypoglycaemia.
25
In non-diabetic
individuals it takes around 30 minutes for mood to be restored to
baseline following experimental hypoglycaemia.
23
Motivation is another important determinant of performance,
and this has been assessed during hypoglycaemia using the
Dundee Stress State Questionnaire.
26
Motivation declined as testing
progressed, both in the experimental and control arms. Reduced
motivation was apparent in the hypoglycaemia arm, and perceived
workload was higher.
Negative mood, poor motivation, and anger during hypo-
glycaemia may have an adverse effect on many activities
including sport, recreation, interpersonal relationships and work
performance. These emotional changes may also have an impact
when using experimentally induced hypoglycaemia to test cognitive
function, which cannot be tested in isolation. The profound effect
that hypoglycaemia exerts on mood and emotions is frequently
overlooked and may contribute to the development of chronic
anxiety states or depression.
Factors which may moderate cognitive effects
A wide inter-individual variation in cognitive dysfunction is present
during hypoglycaemia, although on repeat testing it remains
relatively stable within the same subject. A number of factors may
modify an individual’s cognitive performance during hypoglycaemia,
although this has seldom been explored. These factors influence
the degree to which an individual becomes cognitively impaired
during hypoglycaemia, and the glycaemic threshold at which this
commences. They may influence the risk of progression to severe
hypoglycaemia, which is more likely to occur if cognitive function
becomes severely impaired before an individual perceives the
onset of hypoglycaemic symptoms and can initiate self-treatment.
However, in people with type 1 diabetes who have impaired
awareness of hypoglycaemia, cognitive function is less affected
during moderate hypoglycaemia (blood glucose 2.5 mmol/l) and
recovery is faster than those with normal awareness.
27
Non-modifiable or fixed factors
A number of patient-related factors can influence cognitive
performance during hypoglycaemia. One of these is gender.
Men with type 1 diabetes appear to experience greater cognitive
impairment during hypoglycaemia than women.
6,28
High intelligence
quotient (IQ) was anticipated to be potentially protective, but when
24 nondiabetic patients with differing IQ levels were studied,
29
those
with higher IQ had a greater deterioration in cognitive function.
Age is an important factor that has not been studied adequately,
because of ethical restraints to exposure of elderly people to
experimental hypoglycaemia.
Diabetes-related factors
Diabetes per se may influence how a person responds to
hypoglycaemia, and several studies have compared adults with
type 1 diabetes to non-diabetic volunteers. Similar effects were
seen on working memory
9
and attention.
30
However, in one study
10 adult males with type 1 diabetes performed more poorly on a
battery of cognitive tests than 12 healthy non-diabetic volunteers,
31
although cognitive function at baseline was similar between the
two groups. Psychomotor function was found to be less affected
in those with type 1 diabetes.
18
Various factors might explain these
observed differences including small sample size, differences in
experimental protocol, the cognitive tests that were applied and
the magnitude of hypoglycaemia that was induced. It is possible
that differences between the participants with type 1 diabetes had
an influence, such as their prevailing glycaemic control or their state
of hypoglycaemia awareness.
Glycaemic control was not shown to influence the effect of
hypoglycaemia on cognitive function,
6
or the glycaemic threshold
at which cognitive impairment commenced.
32
However, one study
that used auditory p300 event-related potentials to assess cognitive
function in subjects with type 1 diabetes (7 with strict glycaemic
control and 11 with poor control) found the p300 amplitude was
significantly reduced at a blood glucose of 2.2 mmol/l only in those
with poor control.
33
The effect of impaired awareness of hypoglycaemia has been
investigated in two studies, the earlier of which
34
compared
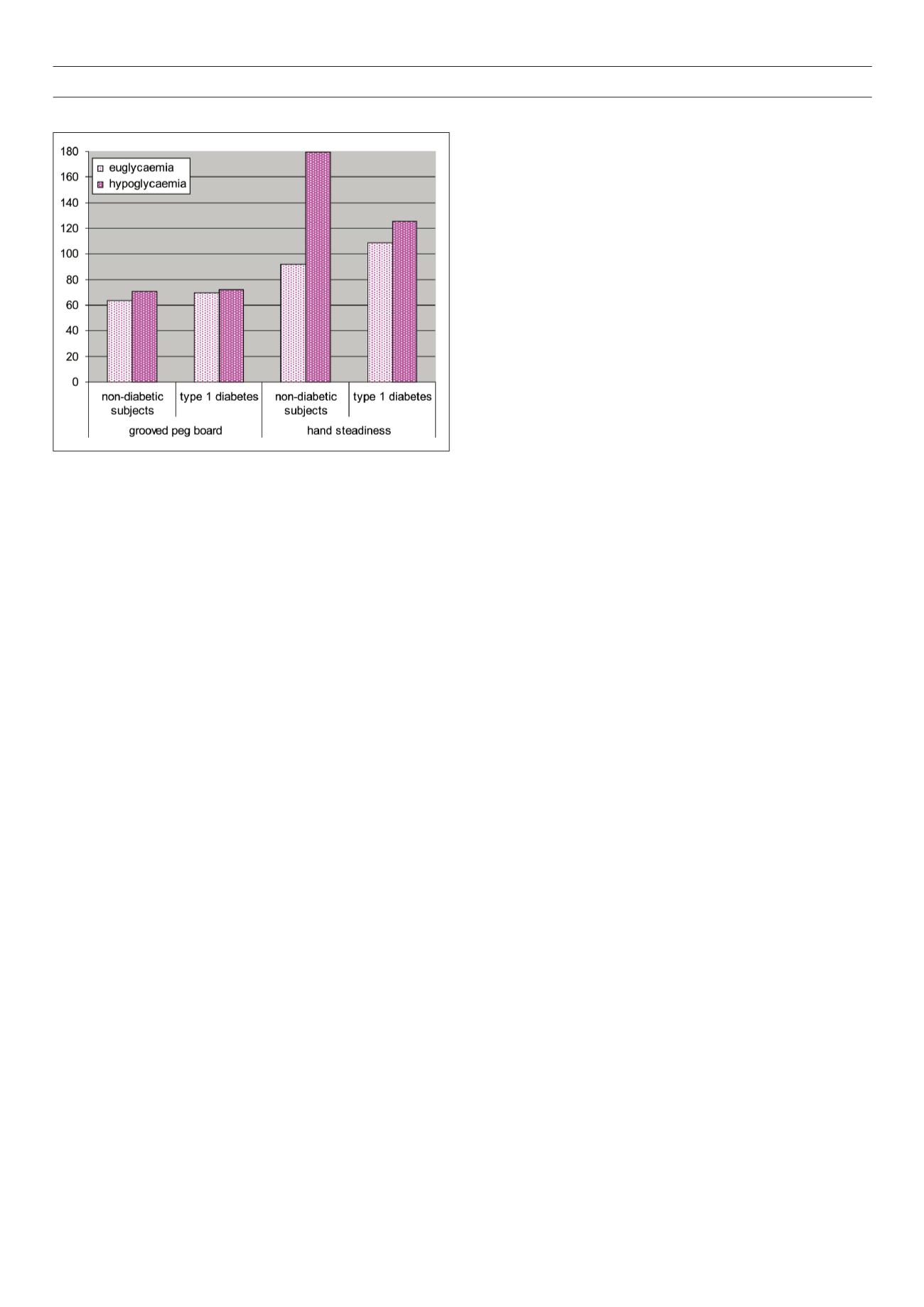
Fig 3.
Results of grooved peg board and hand steadiness tasks in 20 non-diabetic
and 16 subjects with type 1 diabetes during euglycaemia and hypoglycaemia
from Geddes
et al
.
18
Significant difference in performance was observed in non-
diabetic subjects, but not in those with type 1 diabetes.


