VOLUME 11 NUMBER 3 • SEPTEMBER 2014
117
SA JOURNAL OF DIABETES & VASCULAR DISEASE
REVIEW
French lilac
(Galega officinalis)
may be useful in the prevention of
the development of AGEs. The Panax
quinquefolium
(Linnaeus)
[Araliaceae] extracts, a phyto-oestrogen derived from
Vitis vinifera
(Linnaeus) [Vitaceae] (resveratrol), curcumin from
Curcuma longa
(Linnaeus) [Zingiberaceae] and glycosides from
Stelechocarpus
cauliflorus
(RE Fr) [Annonaceae] have also been reported to inhibit
formation of AGEs or RAGE.
50-56
Diabetic nephropathy
Renal disease is a common andoften severe complicationof diabetes,
with the majority of patients with 18 years’ duration showing signs
of diabetic renal involvement.
57
In general, about one in three
patients with type 1 or 2 diabetes develops ESRD which proceeds
to DN, the principal cause of significant morbidity and mortality in
diabetes.
8
The onset of DN is associated with a progressive rate of
decline in renal function, urinary albumin excretion and glomerular
filtration rate. For purposes of this discussion, DN is used as a
generic term referring to any deleterious effect on kidney structure
and/or function caused by diabetes mellitus.
Management of diabetic nephropathy
World Health Organisation data report age-standardised death rate
for diabetics in South Africa is 85 per 100 000 compared with 18
in the USA and six per 100 000 in the UK.
3
The principal reason for
the high mortality rates in South Africa is renal failure as a result of
DN. Some 30 to 40% of diabetics develop nephropathy, which is
the leading cause of ESRD.
14
DN progresses through five well-defined stages.
58
Stage 1 is an
increase in GFR, which progresses to the clinically silent stage 2, in
which hyperfiltration is associated with hypertrophy. Stage 3, or initial
nephropathy, is typified by microalbuminuria, modest increases in
blood pressure and a reduction in GFR. Stage 4 sees macroalbuminuria,
raised blood pressure and progressive reductions in GFR, leading to
stage 5 or ESRD when renal-replacement therapy is required.
ESRD is managed in developed countries by renal replacement
therapy (RRT), such as dialysis and transplantation. In developing
countries, however, kidney failure rates are double those in the
West because access to RRT is severely limited by its high cost to
patients.
13
The figures are stark: 70% of patients in a Nigerian study
were able to afford dialysis for only one month, with less than 2%
having sufficient resources to remain on dialysis for more than 12
months.
59
Access to RRT is virtually impossible for the rural poor.
12
Current conventional diabetes therapy using blood glucose-
lowering medications has limitations in averting renal complications.
Progression towards ESRD may be slowed in part by strict control of
blood sugar levels and blood pressure, a reduction in dietary protein
intake and inhibition of the renin–angiotensin system. Consequently,
drug developmental strategy should target these metabolic pathways
for the prevention of progression to ESRD, which proceeds to DN.
Many patients of sub-SaharanAfrica however cannot afford these
expensive drugs. Hence there is an urgent need to find affordable
treatments which are effective in slowing the progression of DN.
Medicinal plants in the management of diabetic kidney
disease
Ethno-medicinal plants have traditionally been used for the
treatment of diabetes and its complications. In fact, current pre-
clinical and clinical studies have demonstrated that many have
beneficial effects on some processes associated with reduced renal
function in experimental animals.
60-62
The active phytochemicals
responsible for their activities have also been identified.
Our research has established the therapeutic and pharmacological
properties of a number of ethno-botanical herbs traditionally used
in the management of diabetes mellitus by African communities.
15
Observations indicate that some herbal extracts contain compounds
that could be effective in mild diabetes mellitus or in cases of impaired
glucose tolerance (Fig. 1). These are likely to have a positive impact
on glucose homeostasis in diabetic patients.
Investigations from our laboratory have also examined whether
herbal extracts could lower blood pressure or improve the impaired
renal and cardiovascular functions often seen in diabetes. The results
suggest that while some extracts such as
Hypoxis hemerocallidea
corm aqueous extract (APE) had hypoglycaemic effects, they may
have deleterious effects on kidney function. Gondwe
et al
. found
that APE increased renal fluid output and electrolyte retention, and
reduced glomerular filtration rate,
32
neither of which are desirable
in diabetes mellitus.
In contrast, other studies from our laboratories have shown
that Opuntia megacantha leaf extract, which had hypoglycaemic
effects, reversed the inability of the kidney to excrete Na+ in STZ
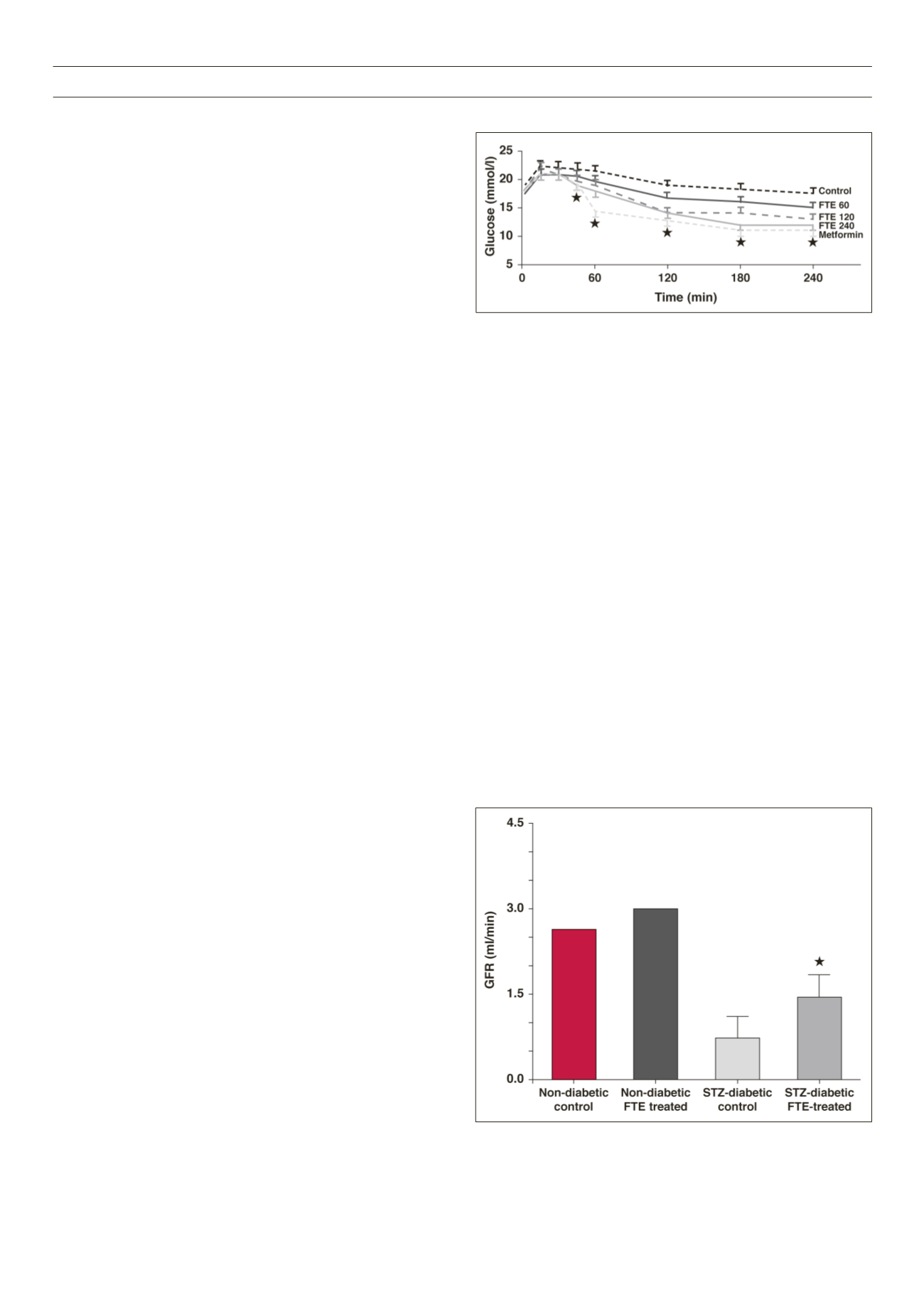
Fig. 1.
Oral glucose tolerance test in STZ-diabetic rats showing dose-related
reduction in plasma glucose levels following treatment with F thonningii bark
ethanolic extracts (FTE, 60–240 mg/kg) comparable to that induced by met-
formin (500 mg/kg).
17
Statistical comparison of the differences between the con-
trol and experimental group means was performed using one-way analysis of
variance (ANOVA) followed by Tukey-Kramer multiple comparison test. A value
of
p
< 0.05 was considered significant.
Fig. 2.
Sub-chronic treatment with F thonningii bark ethanolic extracts (FTE)
every third day increased glomerular filtration rate in STZ-diabetic rats.
63


