


















 37 / 56
37 / 56

VOLUME 13 NUMBER 1 • JULY 2016
35
SA JOURNAL OF DIABETES & VASCULAR DISEASE
RESEARCH ARTICLE
intolerance, questions arise with regard to the possibility of a
connection between under-nutrition and DM.
In general, this study highlights the need to undertake
population-based studies in all districts in the country to quantify
the magnitude of NCDs at a national level. It is evident that
there is variation among ethnic groups and locations, as various
factors contribute to the development of disease and other factors
contribute to the perpetuation of diseases.
In order to institute a cost-effective intervention, the specific
factors at play in a given population must be identified. It may not
be appropriate to generalise these findings to refer to the Karamoja
population. These results though are useful in guiding intervention
and preventative measures for the Kasese population, and should
be well received by policy makers in the local government of Kasese,
as well as the ministry headquarters. For example, vegetables and
fruits are grown in large quantities in Kasese, but consumption is
low. Most are sold to the cities. The population is not aware of
the benefits to their health of eating fruit and vegetables. Mass
education to encourage increased consumption of fruits and
vegetables will benefit the population.
A key strength of this study was the use of a representative
sample, with analysis taking into account the complex survey
design. The relatively high response level minimises the likelihood of
selection bias, and the range of factors that were measured should
be a good reflection of those factors in the Kasese population. The
use of WHO standardised protocols, intensive training of data-
collection staff, pre-study testing of procedures, and the close
supervision of staff during data collection all highlight the attention
that was paid to minimising avoidable sources of measurement
error.
Limitations of this study need to be borne in mind. The STEPS
methodology is designed to provide standardised information on
key modifiable risk factors that can be measured in population-
based surveys without resorting to high-technology instruments. It
is not designed to measure total energy intake, dietary fat, dietary
sodium, body fatness or physical activity by objective methods,
such as accelerometry and pedometry. Information on these
factors would have provided a more comprehensive picture of the
relationships we studied. In addition, these cross-sectional data do
not allow age-related differences in BP, blood glucose and total
cholesterol levels to be attributed to ageing, independent of cohort
effects. Assessment of risk factors by age group as well as fasting
blood sugar level for different BMIs would have provided more
insight. Finally, due to lack of power, we were not able to assess
the relationship between underweight and diabetes.
Conclusion
This study provides the first NCD risk-factor profile of people in
the Kasese district, Uganda, using internationally standardised
methodology. Our findings for this predominantly rural sample
provide evidence for health policy-makers as well as district
authorities on lifestyle problems in the population studied. The
burden of more diseases is to be expected if an effective prevention
strategy is not undertaken.
Although even short-term educational programmes have been
shown to be effective in improving lifestyle, a durable education
strategy and cost-saving policies supported by sustained large-
scale media education and school-based educational programmes
could be the starting point for a possible national programme on
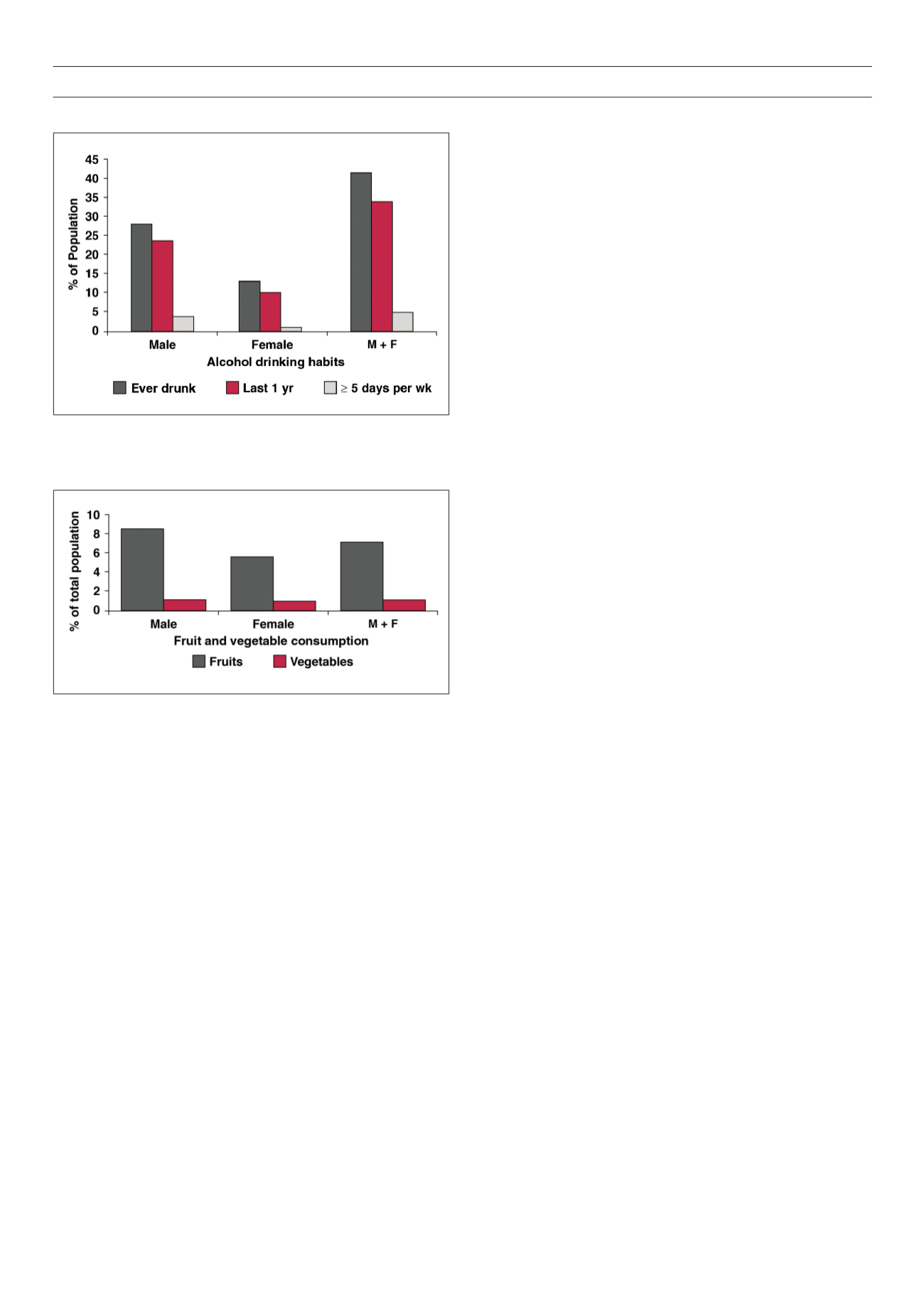
Figure 9.
Alcohol consumption; 41.6% had ever drunk alcohol in life;
34.1% drank in past 12 months; 5.3% of active drinkers ≥ 5 days/wk –
(average number of drinks per day was 3 for men and 2 for women)
Factors not measured in this survey, and which may explain the
observed risk among women, were hormonal status, saturated fat
consumption and salt intake. Also, further studies should be done
to document the proportion of those on treatment whose BP is
under control, as well as the presence of hypertensive heart disease
among those with hypertension.
The second major finding was that the risk profile of this
predominantly rural population of Kasese was markedly different
from that reported previously for the urban and peri-urban
settings.
10-12
The prevalence of raised blood glucose levels (defined
as capillary whole BG of at least 6.1 mmol/l) in 31% of females and
10% of males, DM (13.9% had a family history of DM, 2.9% were
diabetic), raised BMI (15.6% were overweight, 6.7% were obese),
and tobacco smoking (24% had history of smoking with 9.6%
heavy smokers) were markedly higher than previously speculated.
The level of physical activity was surprisingly lower than expected
in this predominantly hilly area, although different definitions of
physical activity could have led to this response. These findings
support the need for regular screening of individuals for NCDs and
their risk factors.
There was a high prevalence of underweight people (29.9%).
When taken together with the observed rates of DM and glucose
Figure 10.
Fruit and vegetable intake; 7.2% of total population ate ≥ 5
servings of fruits per week; 1.2% of total population ate ≥ 5 servings of
vegetables per week