


















 20 / 52
20 / 52

RESEARCH ARTICLE
SA JOURNAL OF DIABETES & VASCULAR DISEASE
58
VOLUME 15 NUMBER 2 • NOVEMBER 2018
In patients with type 2 DM, hypertension is associated with left
ventricular hypertrophy (LVH),
20,21
which is an independent predictor
of cardiovascular events in hypertensive patients with diabetes.
22
Hypertension is also a major risk factor for myocardial infarction
and stroke,
12,23,24
and indeed hypertension is the leading risk factor
for mortality worldwide.
5,25-28
Additionally, hypertension is a major
causal factor of end-stage kidney failure, blindness and non-
traumatic amputation in people with diabetes, where attributable
risks are 50, 35 and 35%, respectively.
16
Unfortunately the majority of people with hypertension in sub-
Saharan Africa do not know they have it, and most are not on
treatment. This reflects the low level of knowledge of the dangers
of untreated hypertension in this population.
10
In sub-Saharan Africa there is still a lack of awareness about the
growing problem of NCDs, which, unfortunately, is often coupled
with the absence of a clear policy framework for prevention
and management.
7
Given the long-term decreased productivity
associated with hypertension among diabetics, identifying and
treating a large proportion of patients has the potential to generate
tremendous social and economic benefits in this region.
5,29-31
In this study we sought to determine the prevalence and factors
associated with hypertension among newly diagnosed adult
diabetic patients in a national referral hospital in Uganda. These
findings are not only necessary, but also contribute to the diagnosis
and management of DM and hypertension in sub-Saharan Africa.
Methods
This study was carried out in the diabetes out-patient clinic, the
medical endocrine ward and the medical emergency ward of
Mulago National Referral Hospital. It is the only national referral
hospital for Uganda and is the teaching hospital for Makerere
University, with a bed capacity of 1 500. Mulago Hospital receives
referrals from all parts of the country including from neighbouring
countries such as Southern Sudan, the Democratic Republic of
Congo and Rwanda. The study population is representative of the
Ugandan diabetic population.
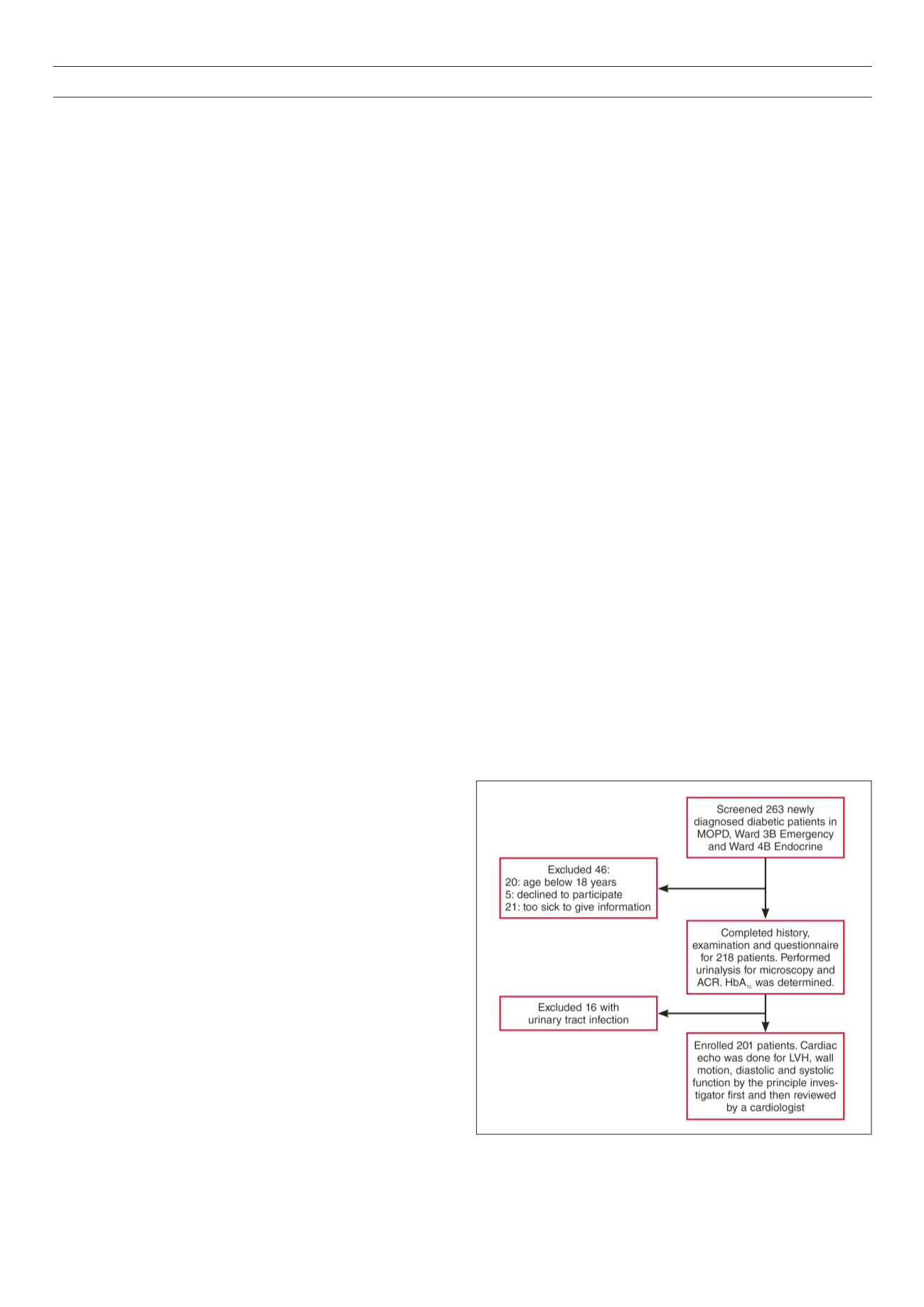
This was a cross-sectional study among 201 newly diagnosed
diabetic patients at Mulago Hospital in Uganda, conducted between
June 2014 and January 2015. All newly diagnosed diabetic patients
aged 18 years and above attending the diabetes clinic or admitted
to the medical wards of Mulago Hospital during the study period,
who met the inclusion criteria and provided informed consent,
were recruited consecutively. We excluded patients with urinary
tract infection in order to avoid confounding in microalbuminuria,
and those who were unable to provide the necessary information.
Fig. 1 illustrates the patient recruitment flow.
Institutional consent was sought from the Department of
Medicine, Makerere University, Mulago National Referral Hospital
and the School of Medicine research and ethics committee
of Makerere University College of Health Sciences. All study
participants provided written informed consent for involvement in
the study. Enrolment was totally free and voluntary, and participants
were free to withdraw at any time without any consequences. The
patients’ records/information was anonymised and de-identified
prior to analysis.
We took a focused history and performed a specific physical
examination to determine biophysical measurements. Information
gathered was entered into a pre-tested questionnaire. We assessed
the following factors: patients’ demographic data, history of
hypertension, age, physical exercise at work and leisure, marital
status, date of diagnosis of DM, drug history, occupation, education
level and last normal menstrual period.
Body mass was measured to the nearest kilogram using a Secco
weighing scale, height was measured in metres using a non-
stretchable tape, and these were used to compute body mass index
(BMI). Waist and hip circumferences were measured and waist-to-
hip ratios were determined for all patients.
Glycated haemoglobin (HbA
1c
) was measured by automated high-
performance liquid chromatography. Other investigations included
urinalysis and microalbuminuria using albumin-tocreatinine ratio.
Echocardiographyparameterswereacquiredusingacommercially
available machine, Phillips HD11XE (Eindhoven, the Netherlands),
with two-dimensional, M-mode and Doppler capabilities. It was
used according to the American Society of Echocardiography
guidelines.
32
Blood pressure was measured using a mercury sphygmomano-
meter, according to the American Heart Association guidelines
for the auscultatory method of blood pressure assessment.
33
The
degree of precision of blood pressure measurement in this study was
± 2 mmHg.
33
Hypertension was defined as present if subjects were
on anti-hypertensive medication, had a history of hypertension and/
or evidence of hypertension (blood pressure ≥ 140/90 mmHg).
Statistical analysis
Data were double entered in a database developed with Epidata
version 3.1, validated, and inconsistences were cleared. The data
were then exported to Stata 13 for analysis. Continuous data
were summarised using measures of central tendency while
categorical data were summarised as frequencies and percentages
and presented in tables. Prevalence was presented as percentages
with their confidence intervals. Comparisons were made using the
Student’s
t
-test for continuous data and chi-squared or Fisher’s
exact test for categorical data.
The outcome was dichotomised as patients having hypertension
or not, then logistic regressionwas used to determine the association
between the predictors and hypertension. This was presented as
Fig. 1.
Patient flow chart.