

















 15 / 42
15 / 42

SA JOURNAL OF DIABETES & VASCULAR DISEASE
RESEARCH ARTICLE
VOLUME 17 NUMBER 1 • JULY 2020
13
of 14 (10.1%) and 11 (7.9%) had scores of two, three and four
(maximum score), respectively. Therefore 57 (41.0%) patients had
a high DNS score, which indicated that a significant proportion of
patients with diabetic neuropathy were symptomatic. In addition,
the DNS score was positively associated with duration of diabetes,
age, blood glucose level and BMI. The DNE score was significant
(> 3) in 21 (15.1%) patients. Using other neuropathy screening
modalities, neuropathy was presumed to be present in 34 (24.5%)
patients using the monofilament, 27 (19.4%) using the tuning fork,
and impaired joint position sense was found in 31 (22.3%) patients.
As shown in Table 5, the risks of developing diabetic foot
ulceration were significant with increasing height (
p
= 0.041) and
BMI (
p
= 0.006) but were not related to age, blood pressure or level
of glycaemic control.
Table 6 shows comparison of peripheral neuropathy as detected
by the various screening modalities. Both the 10-g monofilament
and impaired joint position sense, as defined by the presence/
detection of DPN, had similar sensitivity (24.5 vs 22.3%), while the
sensitivity or detection of DPN was highest with the DNS at 41.0%
and lowest with the DNE at 15.1%.
Discussion
The most important reason for the evaluation of DPN is to assess
the risk of neuropathic foot ulceration, which contributes to 50
to 70% of non-traumatic amputations.
26
The results of this study
showed that the overall prevalence of DPN was 41% among
diabetes patients in south-west Nigeria. This prevalence is higher
than that reported in other populations
27,28
but similar to the 35
and 38% reported in the United Arab Emirates and Saudi Arabia,
respectively,
29-31
who used a similar DNE questionnaire.
The variation in the prevalence of DPN might be due to variation
in the sensitivity and specificity of the various modalities of DPN
diagnosis used in those referenced studies, since the sensitivity and
specificity of the DNS score has been shown to be high when defined
using other standard clinical methods.
6
The DNE questionnaire is
a non-invasive screening test only, and not necessarily diagnostic,
hence it may be less reliable due to its subjectivity.
The present study used the DNS score and DNE, which were
designed by Meijer.
24,32
These scores are simple, reproducible, fast
and easy to perform, and were modified from the widely used
neuropathy symptoms score and neuropathy disability score of
Dyck.
25
The construct validity of these scores in relation to the
SWME and the vibration perception test (VPT) has been studied
previously.
31,32
The correlation between the DNS score and DNE and
NCS was significant (
r
= 0.62 for DNE and 0.51 for DNS).
33
The
VPT is considered the gold standard for diagnosis of DPN and a
significant correlation has been shown between the VPT score and
DNE (
r
= 0.532,
p
< 0.001), DNS (
r
= 0.546,
p
< 0.001) score,
absent tuning-fork sensation (
r
= 0.590;
p
< 0.001), monofilament
sensation (
r
= 0.573;
p
< 0.001) and ankle reflex (
r
= 0.377,
p
=
0.01).
34
The DNS score and DNE are simple clinical scores that are
useful to diagnose peripheral neuropathy in patients with diabetes.
As expected, the DNS, a symptoms score, gives the highest
percentage of detection and diagnosis of DPN. This is not surprising
as it comprises only symptoms, which could be quite subjective
but probably less specific. Also, the DNE, which consists of both
symptoms and examination findings, gave the least value (15.1%)
of all the screening modalities in this study. It is relatively time
consuming compared to the easy-to-use monofilament and tuning
fork, both of which require a total of less than two minutes of
inspection time per individual.
To improve on both the sensitivity and specificity of the screening
methods for the diagnosis of DPN, it has been suggested that two
screening methods, for example the SWME and the tuning fork,
could be combined.
30
Combining the 10-g SWME and 128-Hz
tuning fork makes a practical, highly efficient method suitable for
screening of DPN in type 2 diabetes patients in many hospitals in
developing countries, including primary health centres with limited
diabetes care providers.
Our results show that foot lesions, such as deformity, fissure
and dystrophic nails, frequently occurred among these individuals,
and are features predisposing them to amputation in future if not
detected early. A significant number of diabetic patients in this
study (14.4%) had diabetic foot ulcers (DFUs). This is similar to the
prevalence of DFUs reported from a hospital-based study conducted
in Nigeria,
16
and the 14.3% prevalence reported at the SS Hospital,
Banaras Hindu University, Varanasi, India.
35
This might be due to
similar levels of healthcare management and socio-economic status
of the subjects. Other studies have reported the prevalence of DFUs
in the range of 5.3 to 10.5% among diabetic patients.
36,37
The high prevalence of DPN in this study may have been
due to the relatively older patients, poor diabetic foot self-care
practices, poor health-seeking behaviour and poor diabetes-related
knowledge. Also, the high prevalence of DPN may be related to the
significant numbers of people who resided in the rural areas and
the practice of walking bare foot.
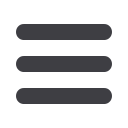
Table 5.
Relationship between neuropathy and the sociodemographic
characteristics of the study participants
Scores
Male,
n
(%)
Female,
n
(%)
Total,
n
(%)
DNS
0
37 (56.1)
45 (61.6)
82 (59.0)
1
12 (18.2)
9 (12.3)
21 (15.1)
2
6 (9.1)
5 (6.8)
11 (7.9)
3
5 (7.6)
9 (12.3)
14 (10.1)
4
6 (9.1)
5 (6.8)
11 (7.9)
DNE
0
40 (60.6)
46 (63.0)
86 (61.9)
1
9 (13.6)
11 (15.1)
20 (14.4)
2
5 (7.6)
5 (6.8)
10 (7.2)
3
2 (3.0)
0 (0)
2 (1.4)
4
3 (4.5)
2 (2.7)
5 (3.6)
5
1 (1.5)
3 (4.1)
4 (2.9)
6
1 (1.5)
3 (4.1)
4 (2.9)
7
1 (1.5)
0 (0)
1 (0.7)
8
4 (6.1)
2 (2.7)
6 (4.3)
9
0(0)
1(1.4)
1(0.7)
DNS: diabetes neuropathy symptoms; DNE: diabetes neuropathy
examination;
n
: number of participants.
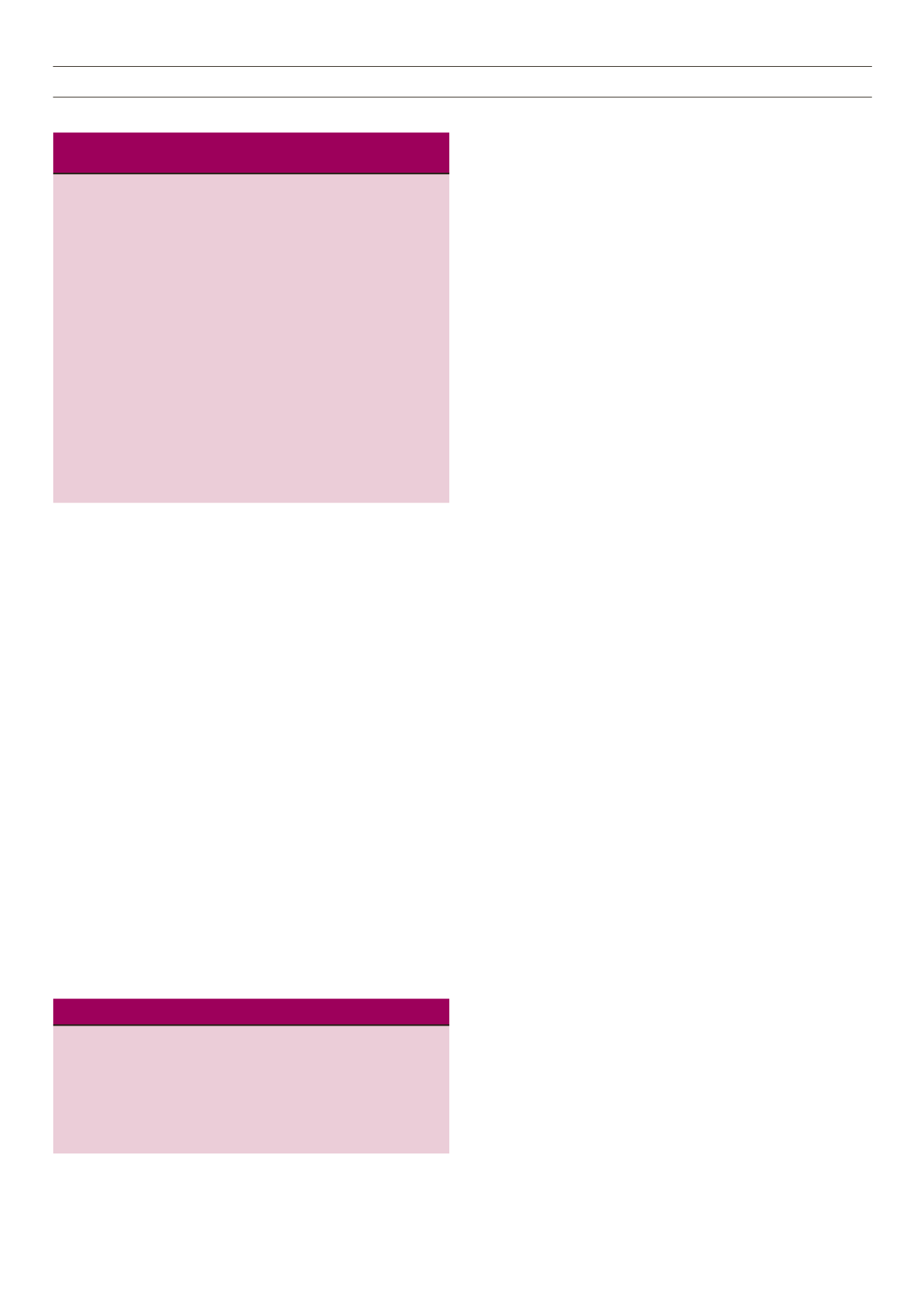
Table 6.
Percentage of neuropathy as identified by different modalities
Modalities
Percentage of neuropathy
n
(%)
DNS
57 (41.0)
DNE
21 (15.1)
Monofilament
31 (24.5)
Tuning fork
27 (19.4)
Impaired joint position sense
31 (22.3)
DNS: diabetic neuropathy score; DNE: diabetic neuropathy examination.