


















 28 / 48
28 / 48

26
VOLUME 12 NUMBER 1 • JULY 2015
RESEARCH ARTICLE
SA JOURNAL OF DIABETES & VASCULAR DISEASE
Fig. 4.
Distribution of no, single and multiple combined lipid abnormalities in
non-very high-risk patients (ESC 2011, SCORE < 10%). TG, triglycerides; HDL-C,
high-density lipoprotein cholesterol; LDL-C, low-density lipoprotein cholesterol;
thresholds for LDL-C are based on the ESC guidelines (2011): SCORE risk 1–4%:
LDL-C ≥ 3.0 mmol/l; patients with SCORE risk 5–9%: LDL-C ≥ 2.5 mmol/l;
patients with CVD, DM, and/or SCORE risk ≥ 10%: LDL-C ≥ 1.8 mmol/l.
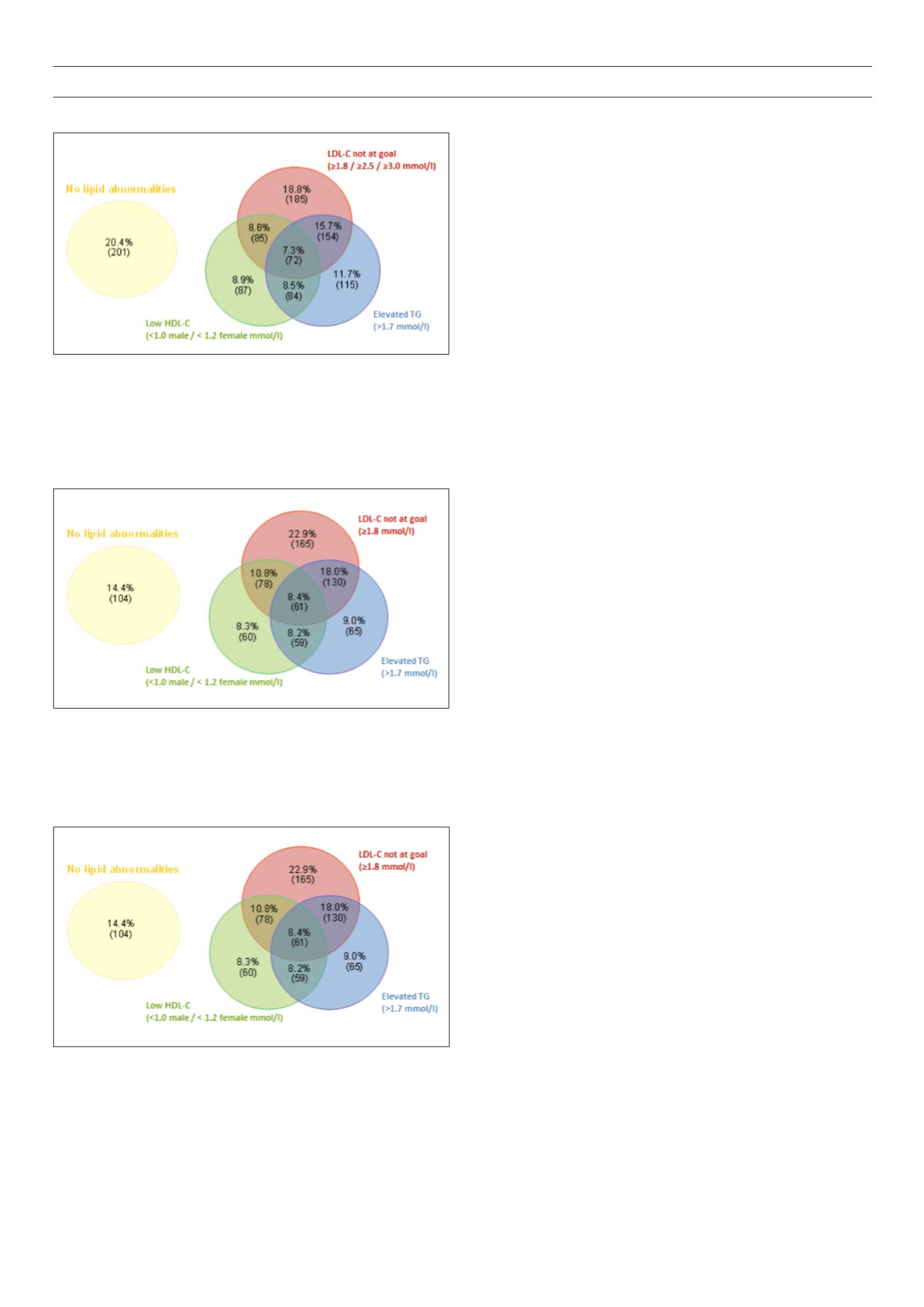
Fig. 5.
Distribution of no, single and multiple combined lipid abnormalities in
very high-risk patients (ESC 2011, SCORE ≥ 10%). TG, triglycerides; HDL-C,
high-density lipoprotein cholesterol; LDL-C, low-density lipoprotein cholesterol;
proportions add up to 100.1% because of rounding; thresholds for LDL-C are
based on the ESC guidelines (2011): SCORE risk 1–4%: LDL-C ≥ 3.0 mmol/l;
patients with SCORE risk 5–9%: LDL-C ≥ 2.5 mmol/l; patients with CVD, DM,
and/or SCORE risk ≥ 10%: LDL-C ≥ 1.8 mmol/l.
Fig. 3.
Distribution of no, single and multiple combined lipid abnormalities for
the total study population. TG, triglycerides; HDL-C, high-density lipoprotein
cholesterol; LDL-C, low-density lipoprotein cholesterol; proportions add up to
99.9% because of rounding; thresholds for LDL-C are based on the ESC guide-
lines (2011): SCORE risk 1–4%: LDL-C ≥ 3.0 mmol/l; patients with SCORE risk
5–9%: LDL-C ≥ 2.5 mmol/l; patients with CVD, DM, and/or SCORE risk ≥ 10%:
LDL-C ≥ 1.8 mmol/l.
By contrast, for the 826 very high-risk patients depicted in Fig. 5,
the majority, 45.4%, had two or more lipid abnormalities (40.2%
had one, 37.0% had two, and the remaining 8.4% had all three).
For non-very high-risk patients, elevated triglycerides were the
largest single abnormality present, appearing in 42.2% of all non-
very high-risk patients. By contrast, among very high-risk patients,
high LDL-C level was the most frequent abnormality, at 60.1% of
all very high-risk patients.
Variables independently associated with dyslipidaemia
Multivariate logistic regression analyses indicated that among the
19 risk factors incorporated into the model, mixed ancestry, along
with history of hypertension, DM and cerebrovascular disease
were among the risk factors strongly, positively and independently
associated with LDL-C levels not being at goal. Having low HDL-C
levels was negatively associated with female gender and increased
alcohol consumption, but positively associated with being treated
by a specialist, increased waist circumference, and presence of
DM. Having elevated triglyceride levels was negatively associated
with age above 70 years, but positively associated with female
gender, obesity, history of DM and peripheral artery disease. The
three variables independently associated with having all three
lipid abnormalities were Asian and mixed-ancestry ethnicity versus
Caucasian ethnicity, and obesity, all of which were positively
associated with not reaching goal (Table 4).
Discussion
In the DYSIS South Africa study we observed marked ethnic
differences in cardiovascular risk profiles and the primary indication
for statin therapy. While about half of Asian and mixed-ancestry
patients had clinically overt CVD, the rate in black patients was less
than 10%. The major indication for statin therapy in black patients
was diabetes, which was present in 71.2% of patients. A family
history of premature CVD was very uncommon (1.8%) in black
patients.
These data are reflective of the epidemiological transition, which
the South African black population is currently undergoing,
6
with
increasing urbanisation and transition to a Westernised lifestyle.
Hypertension, obesity and diabetes are highly prevalent in black
patients while CVD, which results from prolonged exposure to
cardiovascular risk factors, is still relatively uncommon. With further
progression of the epidemiological transition, CVD rates in black
patients are likely to rise and may well match or exceed those
observed in the other ethnic groups if cardiovascular risk factors are
not addressed intensively, both on a population and an individual
level.
The DYSIS South Africa study identified a group of patients at high
cardiovascular risk, with 73.5% of statin-treated patients assessed
to be at very high risk for CVD. Within this very high-risk group,
despite statin therapy, 85.6% had at least one lipid abnormality,
of which a majority had two or more lipid abnormalities. The
most common lipid abnormality was high LDL-C levels, which was
diagnosed in 60.1% of all very high-risk patients.
Moreover, for all patients in the study, 50.5% had LDL-C levels
not at goal, which is comparable with the findings from the
recently published CEPHEUS-SA study and the Canadian/European
cohort of the DYSIS study, and below the levels found in the Middle
Eastern cohort (62%).
24,26,30
Not surprisingly, the metabolic syndrome
was present in 67.2% of the sample, since its components also
contribute to elevated CVD risk.