


















 43 / 52
43 / 52

VOLUME 13 NUMBER 2 • DECEMBER 2016
93
SA JOURNAL OF DIABETES & VASCULAR DISEASE
REVIEW
from chronic gastroenteritis, hypoadrenalism and shortened life
expectancy associated with advanced AIDS.
Despite the scarcity of data from SSA, there are some indications
of overall excess CVD risk factors in HIV-infected patients. Situation
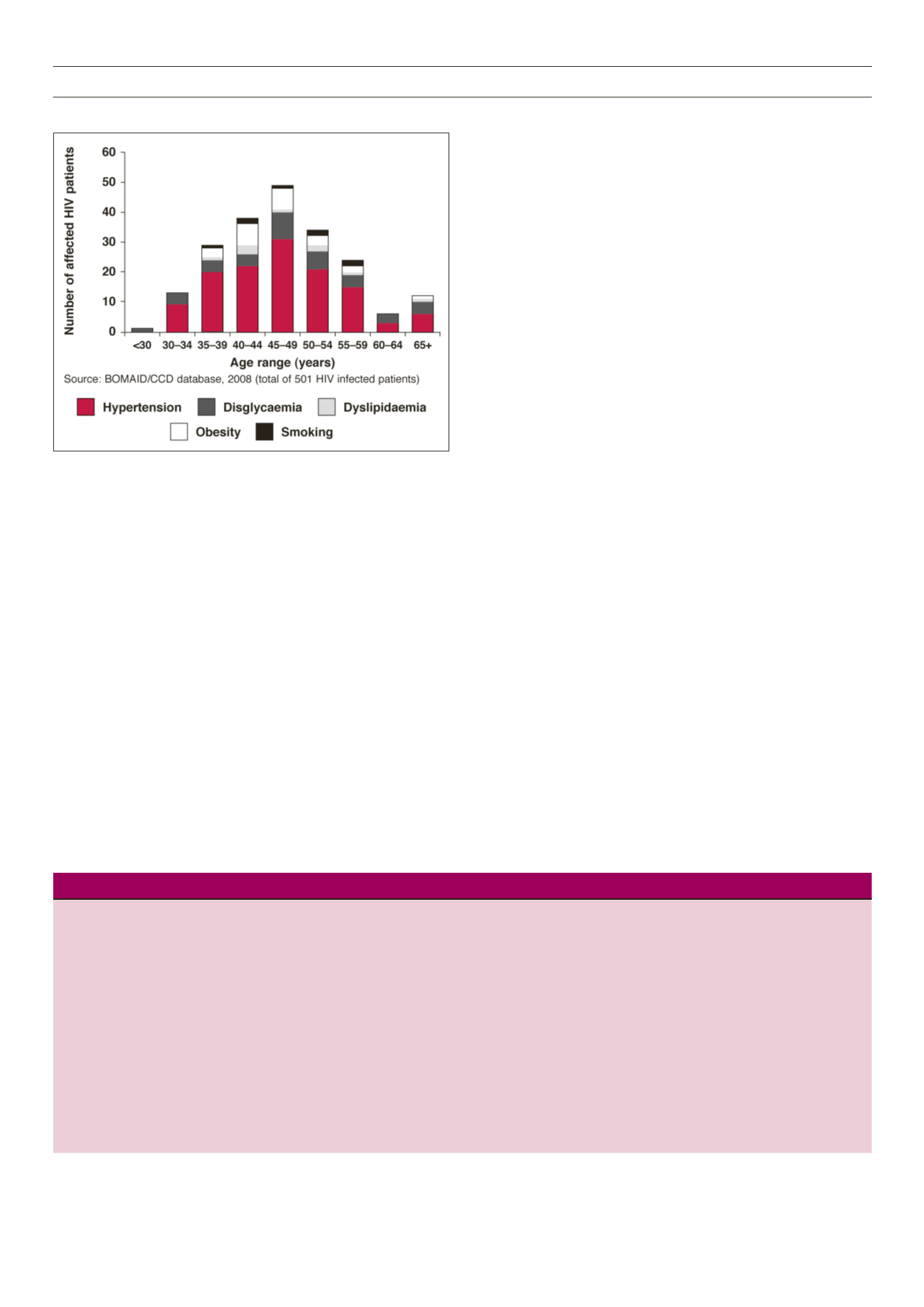
analysis in 2008 of 501 HIV-infected patients from Botswana using
the database of the Botswana Medical Aid Scheme combined with
data from the Centre for Chronic Diseases revealed impressive
clustering of hypertension, dyslipidaemia, obesity, dysglycaemia
and smoking (Fig. 2). The peak age range for the occurrence of
CVD risk factors was about a decade after the peak age for HIV
infection in Botswana.
Given the difficulty of determining whether the observed
increase in CVD risks were due to HIV itself, treatment with HAART
or merely a factor of improved longevity, it would be ideal to
perform case–control studies on the prevalence of CVD risk factors
and the prevalence of arteriosclerotic cardiovascular endpoints such
as IHD, stroke, and peripheral arterial disease in HIV-infected versus
age- and gender-matched non-HIV-infected individuals. Also, a
comparison of pre-HAART and on-HAART HIV-infected patients
would shed light on this grey area. It is important to remember
that the enormous impact of HIV/AIDS does not appear to have
diminished the impact of chronic cardiovascular diseases on
mortality in SSA.
49
Reports on IHD in SSA
There are a few scattered reports of IHD in SSA. Kengne and
colleagues
50
collated a total of 356 cases of SSA patients with
coronary heart disease (CHD) from four selected countries (Ghana,
Cameroon, Senegal and Kenya). They reported a high prevalence
of CHD risk factors, which was not surprising in this selected
population of patients with established CHD. Males outnumbered
females by ratios ranging from 1.3:1 to 6:1, with hypertension in
up to two-thirds of the patients. The report highlighted the fact
that IHD was by no means rare in these African populations.
The African arm of the INTERHEART study showed that
dyslipidaemia, abdominal obesity and tobacco use accounted for
greater population-attributable risk in the overall African population,
whereas hypertension and diabetes were less prominent risk
factors.
51
However, in black Africans, dyslipidaemia was followed by
hypertension, abdominal obesity, diabetes and then tobacco use.
The INTERHEART African study cast doubt on the notion of
protective lipid profiles in blacks, as one reason for implicitly low IHD
prevalence in Africa. High HDL cholesterol levels in black Africans
might be dysfunctional and less protective than generally believed.
However, the findings of the INTERHEART African study were at
slight variance with reports by Ezzati and colleagues who showed
that hypertension, low intake of fruits and vegetables and physical
inactivity accounted for population-attributable fractions for
ischaemic heart disease mortality of 43, 25 and 20%, respectively, in
the Africa region. These were all above the population-attributable
fraction of 15% for high cholesterol.
52
Limitations in diagnostic evaluation of patients with possible IHD
might explain, at least in part, the apparent rarity of IHD in SSA.
This is illustrated by the study on black South Africans by Joubert
and colleagues using data from the Medical University of South
Africa (MEDUNSA) stroke data bank. The study showed increased
prevalence of CHD with improved diagnostic tools.
53
History of angina pectoris or myocardial infarction using the
Rose questionnaire yielded a prevalence of only 0.7% in 741
black patients with stroke, 71% of whom had cerebral infarction.
Resting 12-lead electrocardiography was analysed for the presence
of poor R-wave progression in the precordial leads, the presence of
pathological Q waves and ST–T wave changes using the Minnesota
Fig. 2.
Cardiovascular disease risk factors in HIV-infected patients in Botswana.
Table 5.
Top 10 causes of morality in South African men and women > 60 years in 2000.
COPD = chronic obstructive pulmonary disease.
Cause of death
Percentage (%) in males aged >
60 years [
n
= 71 641]
Cause of death
Percentage (%) in females aged >
60 years [
n
= 73 474]
Ischaemic heart disease
17.2
Stroke
17.7
Stroke
12.2
Ischaemic heart disease
16.0
COPD
8.0
Hypertensive heart disease
9.8
Tuberculosis
6.4
Diabetes mellitus
7.3
Lower respiratory tract infection
5.1
Lower respiratory tract infection
5.3
Hypertensive heart disease
4.2
COPD
4.4
Cancer of airways
4.1
Nephritis
2.8
Diabetes mellitus
4.0
Tuberculosis
2.7
Cancer of prostate
3.1
Asthma
2.4
Cancer of oesophagus
2.8
Cancer of the breast
1.9