


















 10 / 30
10 / 30

RESEARCH ARTICLE
SA JOURNAL OF DIABETES & VASCULAR DISEASE
46
VOLUME 17 NUMBER 2 • NOVEMBER 2020
DM should undergo close follow up and screening for glucose
metabolism disorders.
18
Current recommendations emphasise the
use of OGTT and glycated haemoglobin as screening tests.
26
In a
study conducted in South Africa among patients with CAD, the
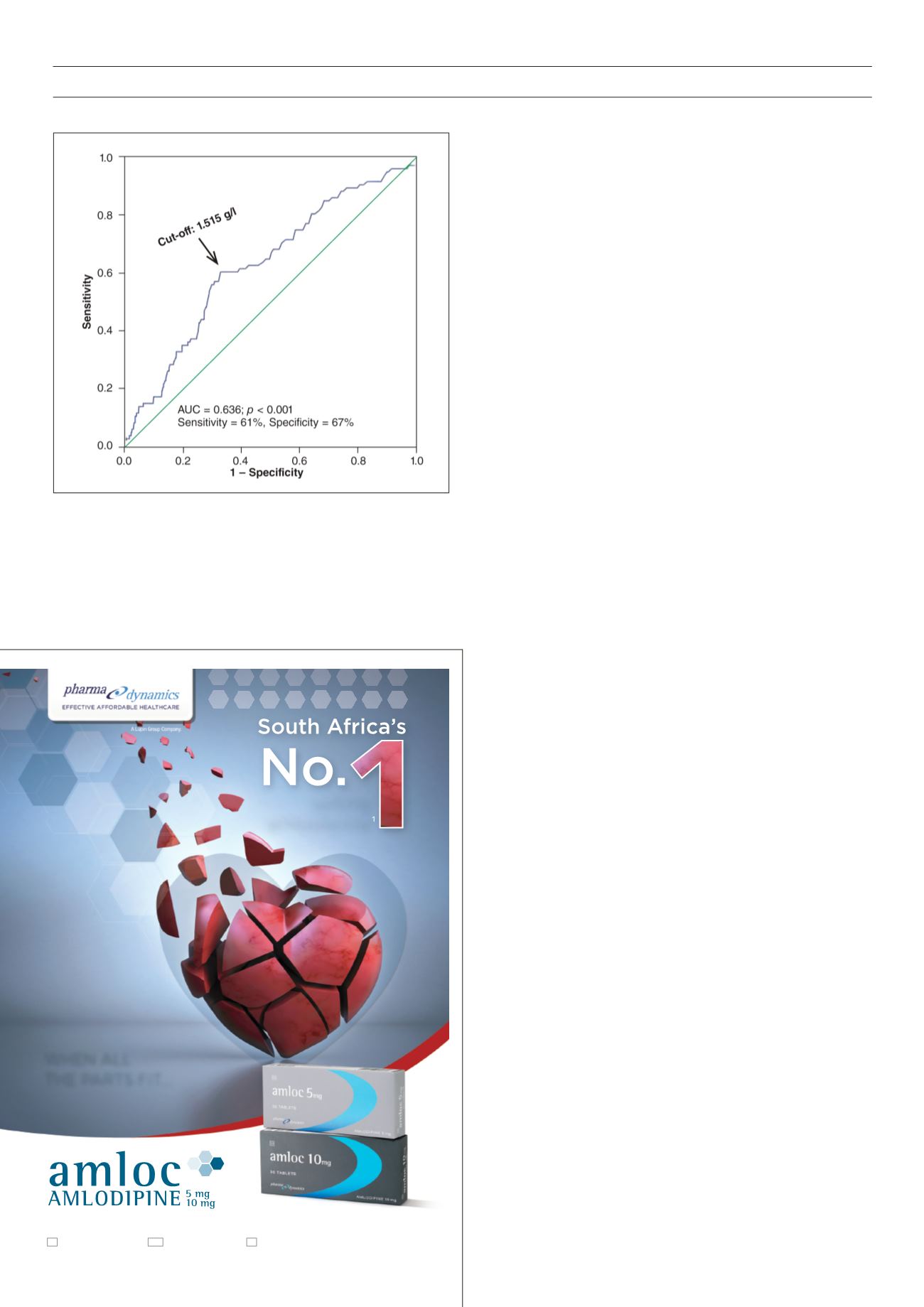
Fig. 1.
ROC curve showing glycaemia cut-off value predictive for in-hospital
death.
rate of IGT measured by OGTT was 30% higher than the rate of
DM (20%).
27
This study included a small sample of patients, but
highlights the need for screening of glucose metabolism disorders
in patients with CAD in our practice.
The other predictors for in-hospital death identified in our study
(age, heart failure, left ventricular dysfunction, sustained ventricular
tachycardia/ventricular fibrillation) are powerful prognostic factors
in ACS patients, consistent with studies in developed countries.
6
Dyslipidaemia appeared to be a protective factor, and this
observation has already been reported.
28
It is mainly the influence
of previous lipid-lowering drugs in patients with high cardiovascular
risk that would have a beneficial effect on mortality rate.
28
Previous
treatments in our study were not specified.
PCI was a protective factor in our series but remarkably, only
in patients without a history of DM in sub-group analyses. First,
the low rate of PCI in our patients with ACS
29
is a potential bias.
Second, CAD patients with DM frequently have multi-vessel
coronary heart disease (28.9%) and complex lesions (39.7%),
30
as in studies conducted in developed countries.
31
Coronary artery
bypass graft surgery is often the technique of choice for complete
revascularisation in patients with DM,
32
but is of limited practice in
sub-Saharan Africa. Finally, DM patients are often high-risk patients
in whom an earlier invasive strategy should be implemented.
However, the excessive admission delays
11
determine the low rate
of PCI, which would weaken its beneficial effect.
Limitations
Our study has some limitations. Incomplete medical records did not
allow us to make a thorough analysis. Glycated haemoglobin was
not available for all patients and was not included in our analysis,
nor was the evolution of blood glucose levels during hospitalisation.
The influence of previous treatments (antidiabetic drugs, statins)
and glucose-lowering treatments given during hospitalisation
(particularly insulin infusion) have not been specified. Finally, the
low rate of coronary angiography did not make it possible to assess
the link between blood glucose levels and the severity of CAD.
Conclusion
This study, carried out in a sub-Saharan African population, shows
that in the acute phase of ACS, admission blood glucose has a
powerful prognostic value on mortality rate, in accordance with
studies conducted in the West. In association with conventional
treatment of ACS, adequate control of blood glucose is an
important treatment target, especially in non‐diabetic patients.
Routine screening for glucose metabolism disorders and follow up
after ACS must be implemented, as recommended.
26
It would be
interesting to determine the rate of IGT and DM in ACS patients
without a history of DM in the post-discharge phase, and assess the
long-term impact of glucose-lowering therapy on morbidity and
mortality rates.
References
1. Kosiborod M, Inzucchi SE, Krumholz HM, Xiao L, Jones PG, Fiske S,
et al.
Glucometrics in patients hospitalized with acute myocardial infarction-defining
the optimal outcomes-based measure of risk.
Circulation
2008;
117
(8): 1018–
1027
2. Zhao S, Murugiah K, Li N, Li X, Xu ZH, Li J,
et al.
Admission glucose and in-hospital
mortality after acute myocardial infarction in patients with or without diabetes: a
cross-sectional study.
Chin Med J
2017;
130
: 767–775.
3. Angeli F, Verdecchia P, Karthikeyan G, Mazzotta G, Del Pinto M, Repaci S,
et al.
selling
amlodipine
AMLOC 5, 10 mg.
Each tablet contains amlodipine maleate equivalent to 5, 10 mg amlodipine respectively.
S3 A38/7.1/0183, 0147. NAM NS2 06/7.1/0011, 0012. BOT S2 BOT 0801198, 0801199. For full prescribing
information, refer to the professional information approved by SAHPRA, 29 September 2017.
1)
IQVIA MAT
UNITS August 2019.
ACF622/10/2019
.
CUSTOMER CARE LINE
0860 PHARMA (742 762)
www.pharmadynamics.co.zaWHEN ALL
THE PARTS FIT...
PERFECTLY.