


















 14 / 30
14 / 30

RESEARCH ARTICLE
SA JOURNAL OF DIABETES & VASCULAR DISEASE
50
VOLUME 17 NUMBER 2 • NOVEMBER 2020
Table 1.
Electrocardiogram parameters
Parameters
Control
STZ
STZ+Mg
Mg
Heart rate (bpm) 233 ± 8
178 ± 14*
218 ± 8#
234 ± 13
R-wave
amplitude (mV) 5.22 ± 0.79 5.67 ± 1.31 6.24 ± 1.17 6.22 ± 0.85
S-wave
amplitude (mV) 1.75 ± 0.27
2.13 ± 0.63
2.35 ± 0.73 0.40 ± 1.38
T-wave
amplitude (mV) 2.12 ± 0.53 2.56 ± 0.67 2.73 ± 0.95 1.76 ± 0.46
QRS interval (s) 0.020 ± 0.003 0.024 ± 0.002 0.026 ± 0.006 0.024 ± 0.003
QT interval (s) 0.062 ± 0.002 0.079 ± 0.009* 0.065 ± 0.005# 0.064 ± 0.006
QTc (s)
0.124 ± 0.006 0.137 ± 0.016 0.119 ± 0.007 0.121 ± 0.009
QTc represents QT interval corrected for heart rate. Values are mean ±
standard error of the mean;
n
= 7–11 per group; *
p
< 0.05 vs control; #
p
<
0.05 vs STZ.
of replicates. Statistical analysis was conducted using Statistica
13. Differences among multiple groups for data with normal
distribution (Kolmogorov–Smirnov and Shapiro–Wilk normality
tests) were evaluated using one-way analysis of variance (ANOVA),
followed by Tukey’s
post hoc
test. For data without normal
distribution, a Kruskal–Wallis test was conducted, followed by
Dunn’s post hoc test. A two-tailed
p
value ≤ 0.05 was considered
statistically significant.
Results
In vivo
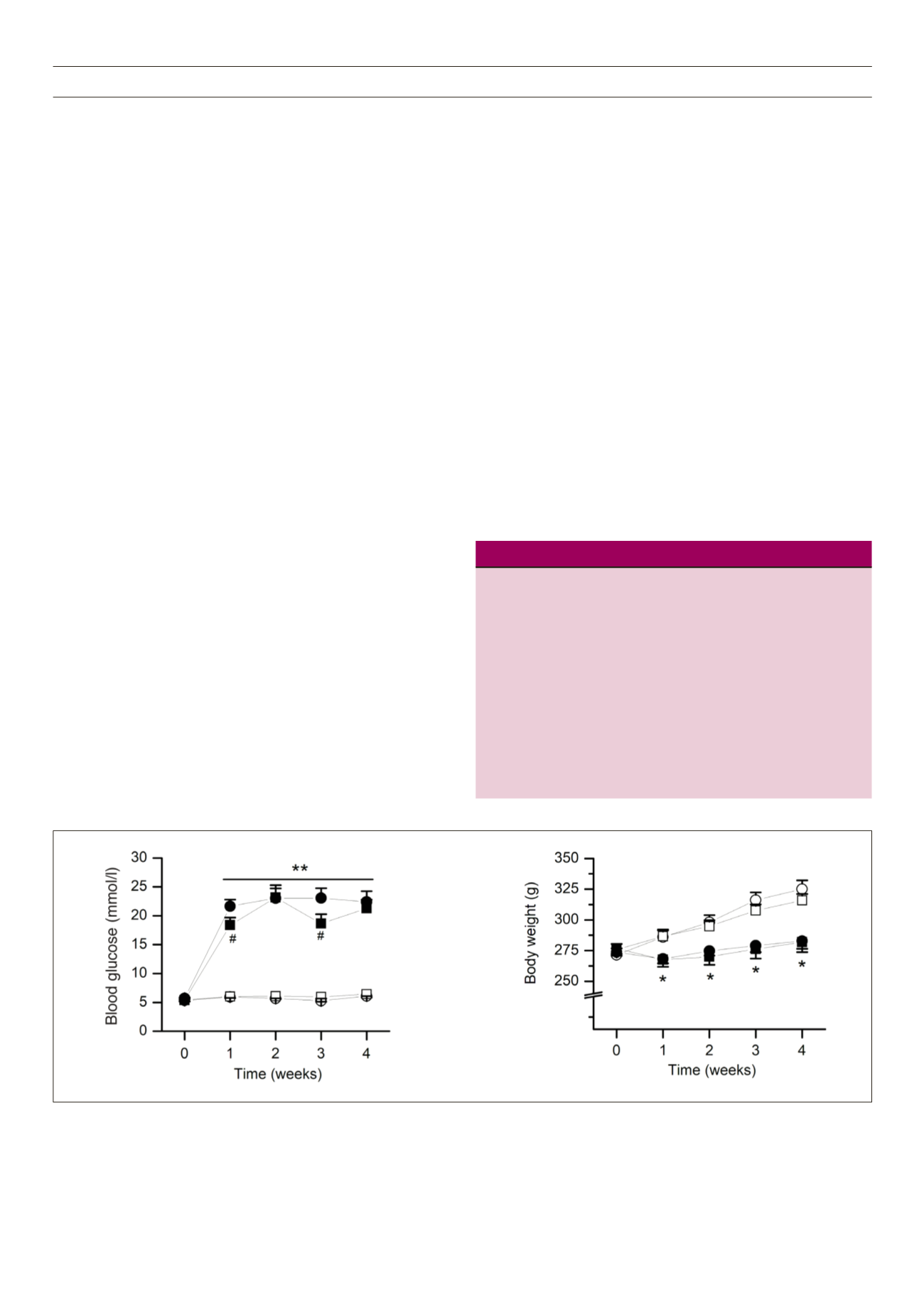
treatment with STZ significantly increased the blood glucose
concentration and decreased the rat body weight (Fig. 1), starting
from the first week after treatment (
p
< 0.05, STZ vs control for
each parameter). Overall, treatment with Mg
2+
did not prevent STZ-
induced hyperglycaemia (
p
> 0.05, STZ + Mg
2+
vs STZ), except for
the transient dips in blood glucose concentration observed in the
first and third weeks (Fig. 1A). Mg
2+
also did not prevent the STZ-
induced loss of body weight (
p
> 0.05, STZ + Mg
2+
vs STZ; Fig. 1B).
Mg
2+
treatment alone had no significant effect on blood glucose
concentration or on body weight (
p
> 0.05, Mg
2+
vs control for
each parameter).
STZ induced a significant decrease in the LVDP (
p
< 0.05, STZ vs
control), and this STZ-induced hypotensive effect was prevented
by Mg
2+
treatment (
p
= 0.03, STZ + Mg
2+
vs STZ; Fig. 2A). Mg
2+
treatment on its own had no significant effect on LVDP (
p
>
0.05, Mg
2+
vs control; Fig. 2A). STZ-treated hearts also exhibited
significant reductions in the indices of LV contraction (+dP/dt
max
)
and relaxation (–dP/dt
max
) as well as in the overall contractility index
(
p
< 0.05, STZ vs control for each parameter; Fig. 2B–D). Among
these changes, Mg
2+
treatment reversed the STZ-induced reduction
of +dP/dt
ma
x and contractility index (
p
< 0.05, STZ + Mg
2+
vs STZ
for each parameter; Fig. 2B, C). Mg
2+
treatment alone had no
detrimental effect on +dP/dt
max
, –dP/dt
max
, or the contractility index
(
p
> 0.05, Mg
2+
vs control; Fig. 2B–D).
In addition, there were no significant differences in coronary
flow rate or in the ratio of heart weight to body weight among
the different treatment groups (Fig. 2E, F). There were also no
significant differences in the diastolic time constant of ventricular
relaxation
(tau)
among the groups (
tau
: 0.043 ± 0.065 s for control,
0.073 ± 0.030 s for STZ, 0.064 ± 0.023 s for STZ +Mg
2+
, 0.080
± 0.033 s for Mg
2+
; values are mean ± SEM,
p
> 0.05,
n
= 6 per
group).
Representative ECG traces recorded on isolated hearts (Fig. 3)
showed typical apex-to-base electrical waveforms that resembled
lead II tracing on a surface ECG recording. Qualitatively, the traces
highlight a reduction in the heart rate of STZ-treated hearts (Fig. 3B)
compared to controls (Fig. 3A), but without noticeable alterations
of the ECG waveform patterns. Summary data of ECG parameters
(Table 1) show that STZ significantly decreased the heart rate and
prolonged the QT interval (
p
< 0.01 vs control for each parameter),
and both these STZ effects could be prevented by Mg
2+
treatment.
Mg
2+
treatment alone had no significant effect on heart rate or
QT interval. There were no significant differences in the R-, S- or
T-wave amplitudes and QRS and QTc intervals among the treatment
groups.
Representative images of ventricular slices stained with either
H&E or Masson’s trichrome are shown in Fig. 4. The H&E images
showed normal cardiomyocyte structural outlines, separated by
extracellular spaces that were relatively free of cellular components
or other infiltrates (Fig. 4A). There were also no apparent distortions
in the arrangement of the myofibrils. There were no significant
Fig. 1.
General parameters. A: Random blood glucose concentration. B: Rat body weight. The parameters were measured weekly in different treatment groups of
rats [
o
, control; •, streptozotocin (STZ);
n
, STZ + Mg
2
+;
q
, Mg
2
+]. Values are mean ± standard error of the mean;
n
= 12–15 per group;
*
p
< 0.05,
**
p
< 0.01 versus
control;
#
p
< 0.05 versus STZ.
A
B