REVIEW
SA JOURNAL OF DIABETES & VASCULAR DISEASE
146
VOLUME 7 NUMBER 4 • NOVEMBER 2010
final cognitive assessment in the HPS was performed by telephone
interview which is less reliable. lastly, the HPS included midlife and
elderly subjects, and thus the above mentioned age-dependent
paradoxical influence of cholesterol level could have been
neutralised.
Summary
There exists a bi-directional association between hypercholesterol-
aemia and cognitive function. In midlife, elevated cholesterol levels
comprise a risk factor for cognitive decline. In elderly subjects,
cholesterol levels decline and are not clearly associatedwith cognitive
impairment. The evidence of treatment of hypercholesterolaemia
by statins solely for prevention of cognitive decline remains unclear.
Hypertension
Hypertension accelerates arteriosclerotic changes through
atheroma formation in large-diameter blood vessels and arteriolar
tortuosity of small vessels.
41
These vascular changes lead to
hypoperfusion producing discrete cerebral infarctions and diffuse
ischaemic changes in the periventricular and deep white matter
(leukoaraiosis) causing vascular cognitive impairment. It has been
suggested that decreased blood pressure (BP) reduces mechanisms
contributing to generalised neurodegenerative changes, which may
account for improvements in impairments on memory tasks.
42
A
postmortem study detected substantially fewer neuropathological
changes (neuritic plaques and neurofibrillary tangle) in medicated
hypertensive patients compared with non-hypertensive controls,
suggesting a salutary effect of antihypertensive therapy.
43
Studies
The results of 28 cross-sectional studies investigating the relationship
between elevated BP and cognition showed conflicting relationships
with positive, negative and J- and U-shaped associations.
44
Cross-
sectional studies, however, are limited in determining the direction
of an association because both exposure and outcome are assessed
simultaneously.
Longitudinal studies have therefore been suggested to be more
appropriate in assessing the relationship between hypertension
and cognitive function. The majority of 22 longitudinal studies
demonstrated elevated BP to be associated with cognitive decline
but some studies showed quadratic, J- and U-shaped relationships
between BP and cognitive performance in addition to three studies
showing elevated BP to be associated with improved cognitive
performance.
44
Observational studies may demonstrate associations but do not
determine causality; the latter being shown only by intervention
studies. Nine completed randomised placebo-controlled clinical
trials investigating the efficiency of antihypertensive treatment
on the development of cognitive impairment have been reported.
Three of these trials had fewer than 100 participants and a
follow-up of less than one year. The remaining six major placebo-
controlled studies showed conflicting results (Table 2): The MRC
trial of hypertension found no significant difference for change in
cognitive function among 4 396 subjects who were randomised
to receive hydrochlorothiazide plus amiloride, atenolol, or placebo
over 54 months.
45
The Syst-Eur Trial investigated, among 2 418
elderly people, whether treatment with nitrendipine, including the
possible addition of enalapril, hydrochlorothiazide or both drugs,
could reduce the incidence of dementia. The follow-up was only
two years as the trial was terminated early because of significant
differences in the incidence of stroke, the primary endpoint. At this
time, active treatment reduced the incidence of dementia by 50%
from 7.7 to 3.8 cases per 1 000 patient-years (21 vs 11 patients,
p
=
0.05), compared with placebo.
46
In the extended phase of this trial
the evidence was reinforced that BP-lowering therapy initiated with
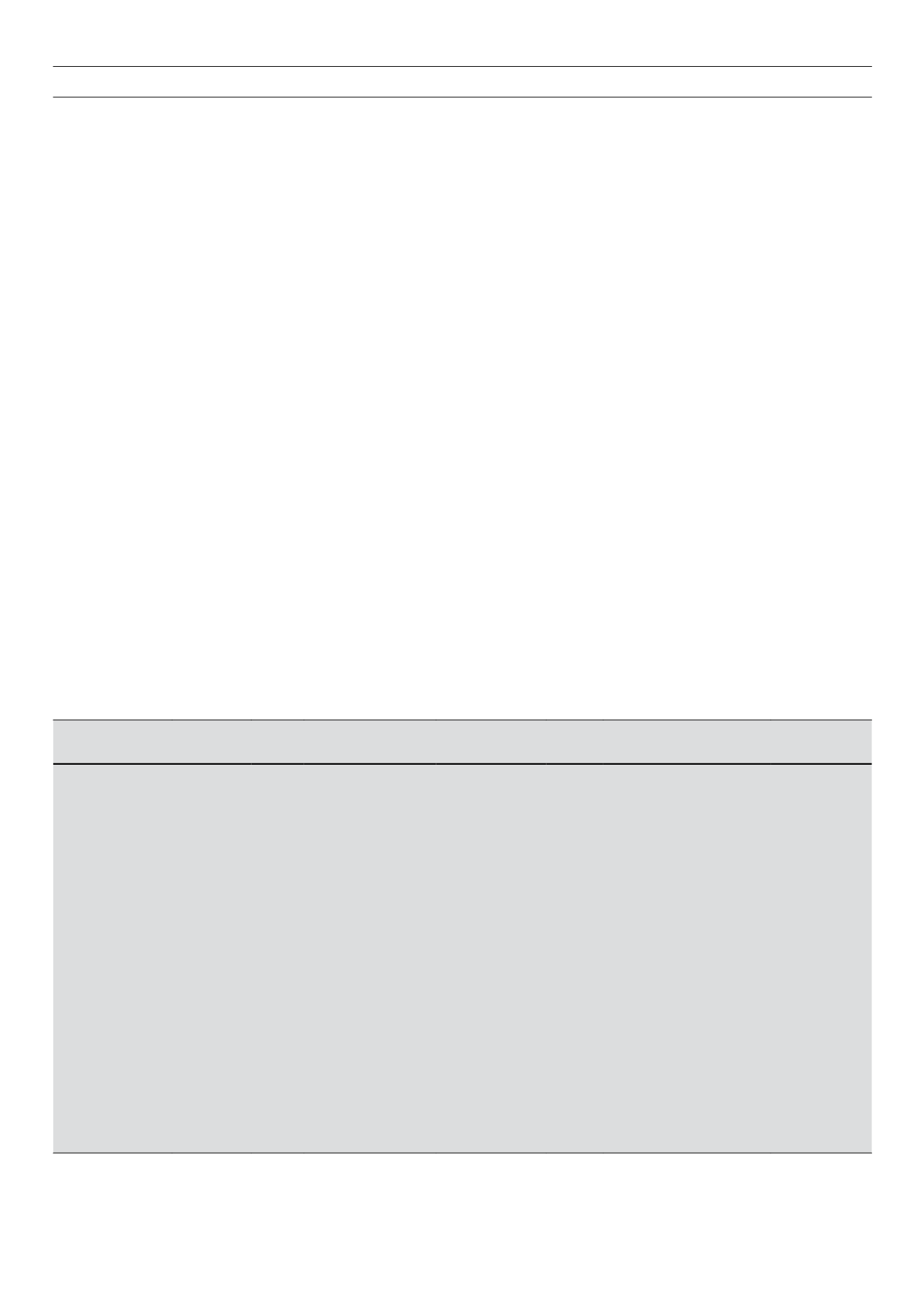
Table 2.
Summary of major placebo-controlled antihypertensive trials assessing protection of cognitive dysfunction.
Study
Participants Mean
age
(years)
Inclusion criteria of
hypertension (SBP
and CBP – mmHg)
Cognitive test
Follow-
up
(years)
Antihypertensive drugs
Result/effect
on cognitive
decline
MRC trial of
hypertension
45
4 396
70.3 Hypertension (SBP
160–209; DBP
<
115)
Paired-associate
learning test, trail-
making test part A
4.5
Hydrochlorothiazide
+
amiloride or atenolol
Not significant
Syst-Eur trial
46,47
2 418
69.9 Isolated systolic
hypertension (SBP
160–219; DBP
<
95)
MMSE
3.9
Nitrendipine
±
enalapril
±
hydrochlorothiazide
HR 0.38 (95% CI
0.23–0.64)
SCOPE
49
4 964
76.4 Hypertension (SBP
160–179; DBP 90–99)
MMSE
3.7
Candesartan
±
hydrochlorothiazide
Not significant
SHEP
48
4 736
71.6 Isolated systolic
hypertension (SBP
160–219; DBP
<
90)
Short care
4.5
Chlorthalidone
±
atenolol or
reserpine
Not significant
PROGRESS
50
6 105
64
Stroke/TIA
MMSE
3.9
Perindopril
±
indapamide
Relative RR 19%
(95% CI 4–32%)
HYVET-COG
51
3 336
83.5 Hypertension (SBP
160–200; DBP
<
110)
MMSE
2.2
Indapamide
±
perindopril
0.86 (0.67–1.09)
CI
=
confidence interval; DBP
=
diastolic blood pressure; HR
=
hazard ratio; MMSE
=
mini-mental state examination; hYVeT-Cog
=
Hypertension Treatment in the
Very Elderly Cognitive function assessment; MRC
=
Medical Research Council; PRogReSS
=
Perindopril Protection Against Recurrent Stroke Study; RR
=
relative
risk; SBP
=
systolic blood pressure; SCoPe
=
Study on Cognition and Prognosis in the Elderly; SheP
=
Systolic Hypertension in the Elderly Program; Syst-Eur
=
Systolic Hypertension in Europe; TIA
=
transient ischaemic attack


