


















 22 / 52
22 / 52

RESEARCH ARTICLE
SA JOURNAL OF DIABETES & VASCULAR DISEASE
72
VOLUME 13 NUMBER 2 • DECEMBER 2016
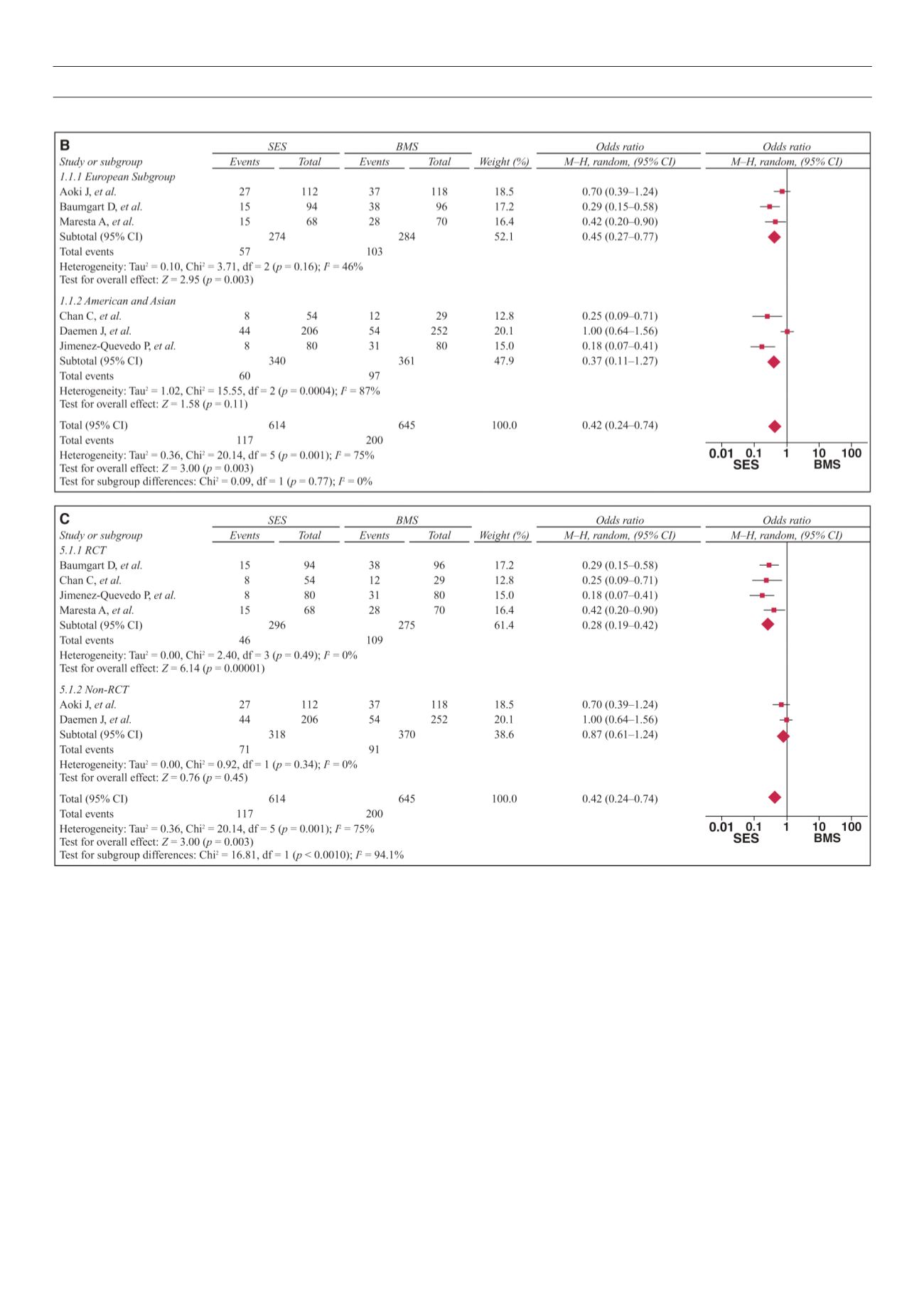
Fig. 6. B
: Forest plots of ethnicity subgroups.
C
: RCT or non-RCT subgroups.
mortality rates and myocardial infarctions,
11
which further proved
the validity of our analysis. The efficacy and safety of SES have
been receiving more and more supportive reports.
30-33
The uniqueness of our analysis and findings is that it proved the
efficacy and safety of SES in CAD patients with diabetes.
Heterogeneity is one major concern with regard to the
validity of meta-analyses.
26,34
Non-homogeneous data can easily
give misleading results. In our study, the
Q
and
I
2
statistics were
performed to test heterogeneity. For all samples, there was
significant heterogeneity for major adverse cardiac events in the
SES and BMS groups.
We further conducted subgroup analysis according to sample
size, ethnicity and study method. It demonstrated that in the
studies where sample size was ≤ 90, method was a RCT and
population was European, the overall major cardiac events were
significantly different between the SES and BMS groups.
Heterogeneity between the studies was decreased after
stratifying the samples. No significant heterogeneity was observed
with RCTs, suggesting an RCT is important for good results. More
high-quality RCTs are therefore warranted.
Another concern for meta-analyses is publication bias, due to
selection of the studies included. In this study, using funnel plots
and Egger’s test,
28,35,36
we found publication bias for overall major
cardiac events, target-lesion revascularisations and myocardial
infarction, but not for overall mortality. Furthermore, the sensitivity
analysis confirmed there was no change if one study was removed
at a time. Although more studies would have produced better
results, overall, our results were statistically reliable.