VOLUME 10 NUMBER 1 • MARCH 2013
27
SA JOURNAL OF DIABETES & VASCULAR DISEASE
REVIEW
Altered reflexes, deformities, ulcers or slow-healing wounds
should be excluded.
Foot examination should be carefully performed and the
reflexes checked. Absent ankle reflexes may imply an early motor
neuropathy.
Vibration sense is examined using a tuning fork and soft touch
is examined using a 10-g Semmes Weinstein monofilament. The
responses to pain, touch, pin prick, pressure, cold, heat, vibration
and temporal summation must be checked and graded as normal,
decreased or increased. The positive pain types are classified as
hyperalgesic or allodynic and categorised in accordance with
the dynamic or static character of the stimulus. Pain sensation is
assessed using a sharp object (a pin) and temperature sensation
using a cold probe.
A careful psychosocial history must be taken and the quality of
life of the patient assessed. Depression, anxiety and sleep disorders
must be excluded, and if present will direct the physician to adopt
specific modes of treatment of the pain.
It is important to remember that although patients may experience
considerable pain, the examination of the peripheral nervous system
may be completely normal, although it is common to find some
distal sensory loss. Likewise, tests such as nerve conduction studies
and electromyography are typically normal in this condition.
Neurophysiological testing using nerve conduction testing and
electromyography are frequently used in suspected disorders of the
peripheral nervous system. Polyneuropathies and focal nerve lesions
with only small-tier involvement can have normal nerve conduction
velocity and electromyography despite significant nerve damage
and neuropathic pain. Other modalities used in the diagnostic work
up include quantitive sensory testing, autonomic nerve testing and
skin biopsy.
4
Goals of neuropathic pain treatment
8,9
Treatment of neuropathic pain must be individualised. The primary
goal is the reduction of pain. If it is not possible to eliminate pain,
as is often the case, treatment should focus on ameliorating the
pain. Secondary goals include improvement in physical function,
reduction in affective distress and improvement in quality of
life. Achieving these goals is dependent on making an accurate
diagnosis of any underlying aetiology.
The first step in the management of PDPN is to optimise
glycaemic control. In the DCCT, strict control of the blood sugar
not only decreased the incidence of neuropathy, but also slowed its
progression by 57%.
2
Concomitant chronic medical conditions and treatment of
these conditions must be taken into account. Individual risks,
such as history of previous drug abuse or suicide attempt must be
considered. Cost of treatment should be discussed with the patient
and must be affordable.
The drug regimen must be carefully planned with the patient
and potential side effects addressed. Fears regarding possible
negative outcomes and lack of efficacy of the treatment should be
discussed.
Treatment recommendations are often given as tier I, II or III
depending on evidence supported from three or more, two or
one randomised clinical trial, respectively. Safety data, special
considerations, co-morbid conditions, and cost are important
considerations in choosing a particular drug.
1,10-17
Choosing treatment options
By understanding the site at which different drugs act, a regimen
can be chosen that is complementary and where treatment is aimed
at specific sites of pain control.
18,19
Opioids are μ-receptor agonists
and bind to μ-opioid receptors, to stop disinhibiton. Opioids used
for neuropathic pain therapy include oxycodone and tramadol.
Selective serotonin–norepinephrine re-uptake inhibitors (SNRIs)
aid in neuropathic pain therapy as they inhibit the re-uptake of
serotonin and help increase the levels of serotonin available.
Duloxetine is approved for treatment of diabetic peripheral
neuropathic pain.
Tricyclic antidepressants (TCAs), including amitriptyline, work
like SNRIs, blocking the re-uptake of serotonin. Additionally, TCAs
serve as sodium channel blockers, which may aid in neuropathic
pain treatment.
Alpha-2
δ
-ligands, including pregabalin and gabapentin,
are calcium channel blockers used in neuropathic pain therapy.
These help decrease levels of neurotransmitter involved in central
sensitisation.
Older sodium channel blockers (anticonvulsants and anesthetics)
aid in modulating the release of excitatory amino acids, including
glutamate, and can be used in neuropathic pain therapy. Vanilloid
receptors sense extreme heat and can be activated by capsaicin to
reduce neuropathic pain.
The choices for individual patients must take into account
patient factors such as co-morbidities, other medication taken by
the patient, goals of treatment, adverse-event profiles of agents,
drug interactions, and cost and availability of the drugs. The choice
of first-tier agents used to treat pain is based on positive results
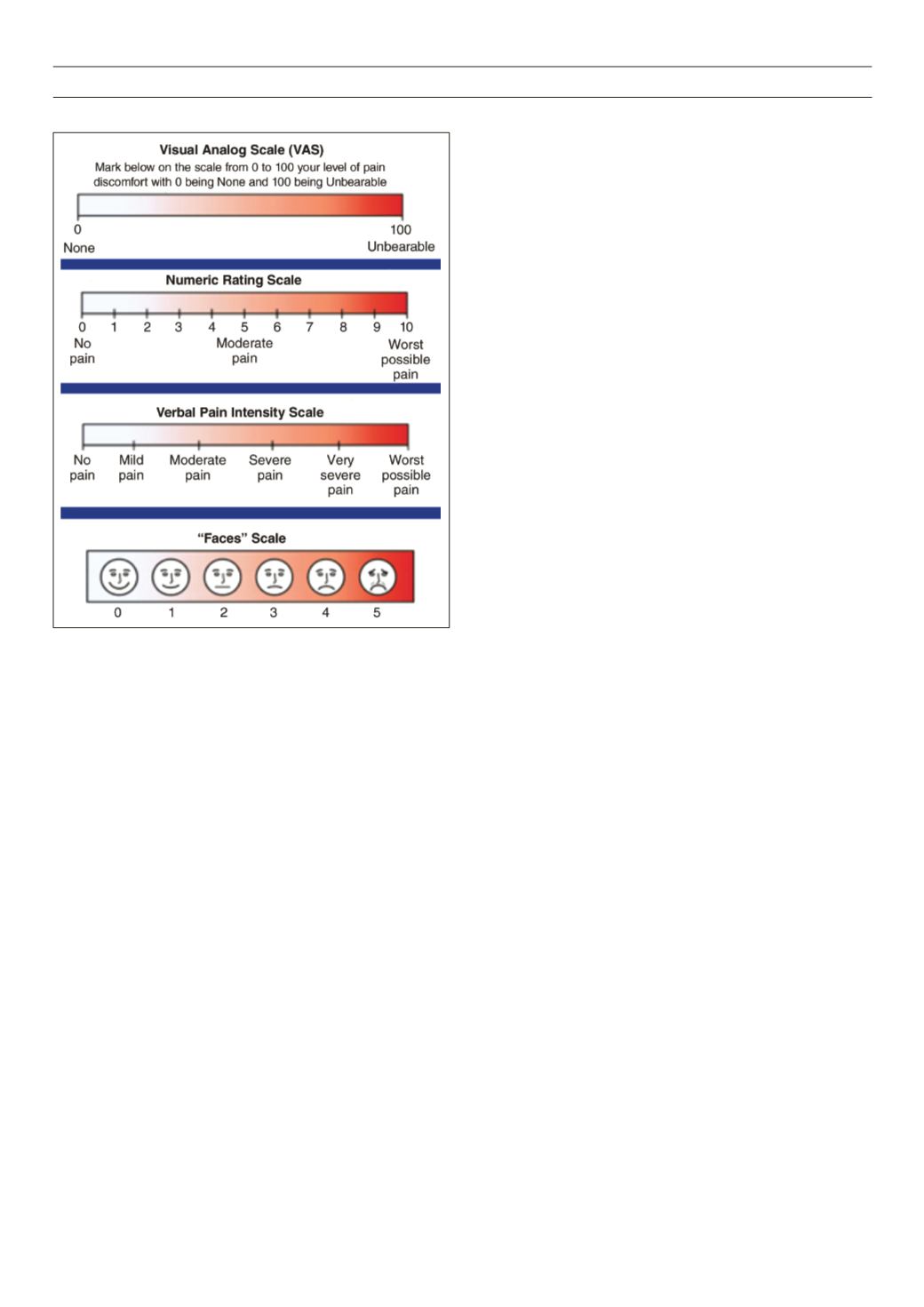
Figure 6.
The Likert pain scale.


