VOLUME 10 NUMBER 1 • MARCH 2013
19
SA JOURNAL OF DIABETES & VASCULAR DISEASE
REVIEW
in type 2 diabetes – including low HDL concentrations, the
predominance of small dense LDL and high postprandial fat levels
– might arise as sequelae of hypertriglyceridaemia.
11
Against this background, normotriglyceridaemia type 2 diabetes
patients with microalbuminuria are almost three times more likely to
show postprandial triglyceridaemia than normoalbuminuric diabetic
patients. (This study excluded patients with macroalbuminuria or
abnormal liver or thyroid function.
13
) Hypertriglyceridaemia is also
associated with prothrombotic haemostatic changes,
13
although
several mechanisms contribute to enhanced prothrombosis in
diabetes, including impaired fibrinolysis and coagulation, as well as
endothelial and platelet dysfunction.
14
Hypertriglyceridaemia-related risk in diabetes
Compelling evidence suggests that hypertriglyceridaemia increases
CVD risk in diabetes. For instance, Schulze
et al
. followed 921
women with type 2 diabetes who did not show CVD at baseline
for 10 years. Of these, 122 women developed incident CHD.
At baseline, the mean age (60.6 years) and the mean fasting
triglyceride level (2.56 mmol/l) among women who developed
CHD differed significantly from those who remained free of CHD
(58.0 years; 2.15 mmol/l). The relative risk of CHD (adjusted for
various confounders including age, hypertension, BMI and aspirin
use) showed a trend towards an increased risk from low (median
0.98 mmol/l) to high (median 3.45 mmol/l) levels of fasting
triglycerides (relative risk 1.42; 95% CI 0.79–2.54), although this
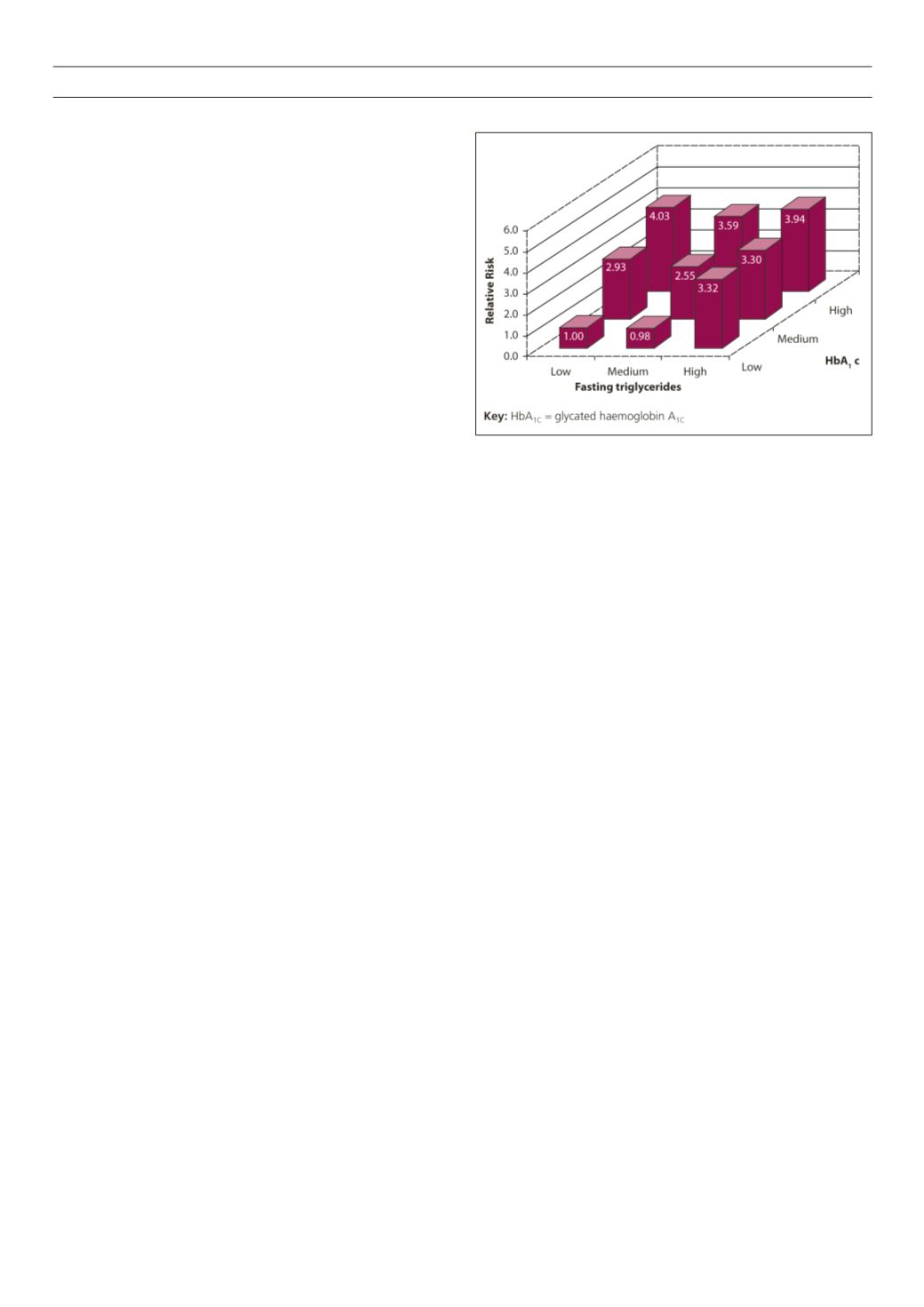
was not statistically significant. High levels of fasting triglycerides
increased CVD risk among women with low HbA
1C
concentrations.
The relative CVD risk comparing the bottom and top fasting
triglyceride tertiles was 3.32. This association was not present
among women with high HbA
1C
concentrations (Fig. 1), possibly
suggesting that poor glycaemic control may mask the effects of
HDL and triglyceride levels.
5
Laakso
et al.
followed 153 men (mean age 56 years) and 160
women (meanage58 years)withnon-insulin-dependent diabetes for
up to seven years. Total triglyceride levels > 2.3mmol/l approximately
doubled the risk of age-adjusted death from CHD (OR 2.2; 95% CI
1.2–4.0) and all CHD events (OR 1.6; 95% CI 1.0–2.8) compared
with lower concentrations. The independent association between
total triglycerides and CHD events disappeared on multivariate
logistical regression analysis that controlled for high LDL (< 4.3
mmol/l) and HDL (> 1.2 mmol/l). However, in patients with low LDL
cholesterol (≤4.3 mmol/l; unstandardised
β
-coefficient 1.0266) and
low HDL cholesterol (≤ 1.12 mmol/l; unstandardised
β
-coefficient
0.8129) VLDL triglycerides were significantly associated with CHD
events, suggesting an independent relationship.
6
The Strong Heart Study followed 2 108 Native Americans with
type 2 diabetes and 2 060 non-diabetic controls, all of whom were
free from CVD at baseline. After an average of 9 years, 521 and 145
of the diabetic and non-diabetic patients respectively had developed
CVD. Based on a Cox multivariate regression model, compared with
triglyceride levels < 1.20 mmol/l, men with concentrations of 1.20–
1.98 mmol and > 1.98 mmol were 40% (95% CI 0.94–2.07) and
39% (95% CI 1.00–1.98) respectively more likely to develop CVD,
after adjusting for several non-lipid confounding variables such as
age, BMI, HbA
1C
and insulin use. Compared with triglyceride levels
< 1.28 mmol/l, women with concentrations of 1.28–1.98 mmol
and > 1.98 mmol were 36% (95% CI 0.99-–1.87) and 61% (95%
CI 1.17–2.22) respectively more likely to develop CVD.
7
Figure 1.
Relative risk of coronary heart disease by tertiles of HbA
1C
(%) and
fasting triglycerides (mmol/l)
5
Diabetes and pancreatitis
Chronic pancreatitis causes between 0.5 and 1% of cases of
diabetes, and between 40 and 60% of patients with chronic
pancreatitis, show concurrent diabetes.
15
Hypertriglyceridaemia
may partly account for this overlap. Indeed, hypertriglyceridaemia
causes up to 10% of acute pancreatitis and up to half of gestational
pancreatitis cases.
16
The mechanism linking hypertriglyceridaemia
and pancreatitis remains unclear. However, an increase in pancreatic
free fatty acid levels could induce inflammation. Alternatively,
hyperviscosity due to elevated chylomicron levels could cause
capillary ischaemia and acidosis.
8
Hypertriglyceridaemia tends to be a primary cause of pancreatitis
only at relatively high concentrations. In a Canadian study, 15 of 95
patients (mean age 54.2 years; 73.7% male; 41.1% with diabetes)
presenting with non-acute pancreatitis showed triglyceride levels
> 20 mmol/l (mean 38.1 mmol/l). In contrast, none of the control
group of 91 patients showed pancreatitis despite triglyceride levels
between 10 and 20 mmol/l.
9
Defining hypertriglyceridaemia in type 2 diabetes
There is a broad consensus that very high levels of triglycerides
(typically > 10–11 mmol/l) increase the risk of acute pancreatitis.
9,12,17
There is less agreement about the levels of triglycerides that
increase cardiovascular risk. Indeed, NICE did not set a target for,
or specifically define, hypertriglyceridaemia in the lipid modification
or type 2 diabetes treatment guidelines in a manner analogous to
HDL and LDL. However, a UK consensus panel recently agreed a
quadripartite stratification, based on fasting levels.
18
Desirable: < 1.7 mmol/l
•
Abnormal, moderately high: 1.7–9.9 mmol/l
•
Abnormal, very high: 10–20 mmol/l
•
Abnormal, extremely high: >20 mmol/l.
•
Similarly, Jialal
et al.
, for example, proposed that fasting
triglyceride concentrations of 1.69–5.6 mmol/l represent mild
to moderate hypertriglyceridaemia. Triglyceride levels of at least
5.6 mmol/l indicate severe hypertriglyceridaemia.
19
A consensus
panel suggested a bipartite classification where non-fasting
triglyceride levels ≥ 2 mmol/l and that postprandial levels following


