

















 36 / 42
36 / 42

34
VOLUME 17 NUMBER 1 • JULY 2020
CASE REPORT
SA JOURNAL OF DIABETES & VASCULAR DISEASE
Diabetes predisposes patients to atrial fibrillation
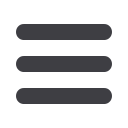
Diabetes also increases the risk for the development of AF. Two
cohort studies, the first based on Framingham data and the
second on a large American register from the Veterans’ Health
Administration Hospitals, have associated diabetes with increased
AF risk. The Framingham data reflected a 40% increased risk of AF
and there was a doubling of risk in the American study (Fig. 4).
5,6
In T2DM patients with AF, there is a substantially increased risk of
death and cardiovascular events. This was shown in the ADVANCE
trial of 11 140 T2DM patients, including 7% with AF. In this study,
AF impacted on the outcome of both all-cause mortality and major
cerebrovascular events over five years (Fig. 5).
7
Fig. 4.
Diabetes predisposes patients to AF.
5,6
Fig. 5.
AF and T2DM frequently co-exist and are associated with subsequent
increased risk of death and cerebrovascular events.
7
The risk for development of AF is further increased in the patient
with CKD and the metabolic syndrome, which is characterised
by dysglycaemic traits other than diabetes (Fig. 6).
8
This stresses
the need for clinicians to screen not only their T2DM patients’
glucose levels, but for all relevant risk factors, and to consider
appropriate interventions, including nonvitamin K antagonist oral
anticoagulants (NOACs) for the management of AF.
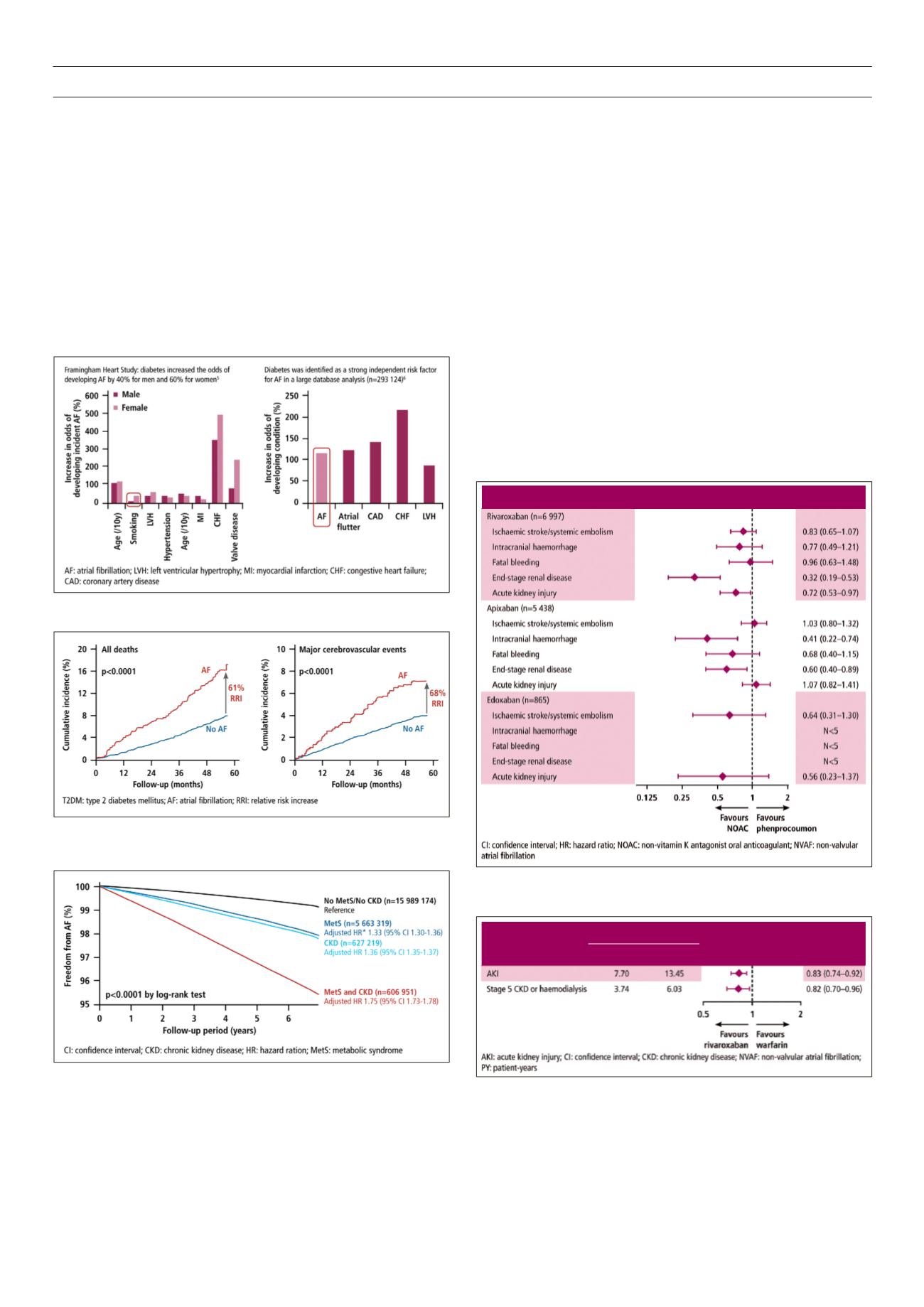
Risk reduction in T2DM patients with AF using NOACs
The RELOADED study of diabetic patients with non-valvular AF
(NVAF) using rivaroxaban showed a trend towards risk reduction
for end-stage renal disease and a slower progression to acute
kidney injury (AKI). There was no increase in ischaemic/systemic
embolism, intracranial haemorrhage and fatal bleeding with the
use of rivaroxaban (Fig. 7).
9
Follow-up of patients, using ICD10 diagnostic codes for diabetes
and AF and prescription information from MarketScan and other
real-world data sets, evaluated progression to renal dysfunction
(AKI, stage 5 CKD or haemodialysis) of those patients newly initiated
Fig. 6.
The metabolic syndrome and CKD increase risk of AF.
8
Kaplan-Meier curves
showing the cumulative event-free survival for AF in
patients classified into four groups based on the presence/absence of metabolic
syndrome and CKD. *The associations were tested using a Cox proportional
hazards model adjusted for age, sex, alcohol consumption, smoking status and
physical activity.
Fig. 7.
RELOADED: Trend towards risk reductions observed in T2DM patients
with NVAF using NOACs.
9
Fig. 8.
Risk of major adverse renal outcomes in diabetic patients with AF
receiving rivaroxaban vs warfarin.
10
Retrospective analysis of US MarketScan
claims data for patients with NVAF and diabetes, newly initiating therapy with
rivaroxaban (
n
= 10 017) or warfarin (
n
= 11 665). Patients with CKD stage 5 or
on haemodialysis were excluded.
NOAC vs phenprocoumon (n=8 545)
HR (95% CI)
HR (95% CI)
Rate per 100 PYs
Rivaroxaban Warfarin
HR (95% CI)
HR (95% CI)