

















 38 / 42
38 / 42

36
VOLUME 17 NUMBER 1 • JULY 2020
CASE REPORT
SA JOURNAL OF DIABETES & VASCULAR DISEASE
Patient and complaint:
68-year-old female, complains of leg pain
and unsteadiness when walking.
Current treatment:
Metformin, amlodipine, atorvastatin.
Medical history:
NVAF, diabetes, hypertension, kidney injury:
eGFR = 43.
Considerations:
It is unclear whether she has peripheral
neuropathy or peripheral arterial disease. Clinical examination
confirms the presence of AF with a heart rate around 70 beats per
minute. She and her family are concerned about her unsteadiness
and have heard that she may need oral anticoagulation.
ANTHONY DALBY
Anticoagulation case study: special considerations in diabetes and CKD
Should she be anticoagulated?
A.
Yes
B.
No
Expert comment
She has confirmed NVAF so we should be guided by the CHA
2
DS
2
-VASc score.
When her age, sex, hypertension and diabetes are taken into account, there
appears to be a strong indication for anticoagulation to prevent her having a
stroke. However, her impaired kidney function needs to be carefully weighed
up against the need for anticoagulants. Many clinicians are guilty of preferring
an act of omission rather than an act of commission, meaning they would
rather avoid anticoagulation and its attendant bleeding risk than reduce the
patient’s risk of stroke.
Having decided to anticoagulate, what should be the choice of
anticoagulant?
A.
Vitamin K antagonist – warfarin
B.
Aspirin
C.
NOAC
Expert comment
In this setting it is inappropriate to consider aspirin at all. Aspirin has little or no
effect on stroke risk and carries as great a risk of bleeding as warfarin. So, our
first decision is whether to use the vitamin K antagonist (warfarin) or a NOAC.
Leaving aside the issues of inconvenience, drug interactions, monitoring and
dose variations with warfarin, we must be aware that NOACs are equal if not
better at preventing strokes in patients with NVAF and also carry a lower risk
of brain bleeds. Though cost is frequently an issue that favours warfarin, we
need to be aware that the best clinical advice is to use a NOAC.
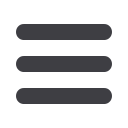
Risk factor
Score
Congestive heart failure/LV dysfunction
1
Hypertension
1
Age > 75 years
2
Diabetes mellitus
1
Stroke/TIA/thromboembolism
2
Vascular disease
1
Age 65–74 years
1
Sex category (i.e. female sex)
1
Maximum score
9
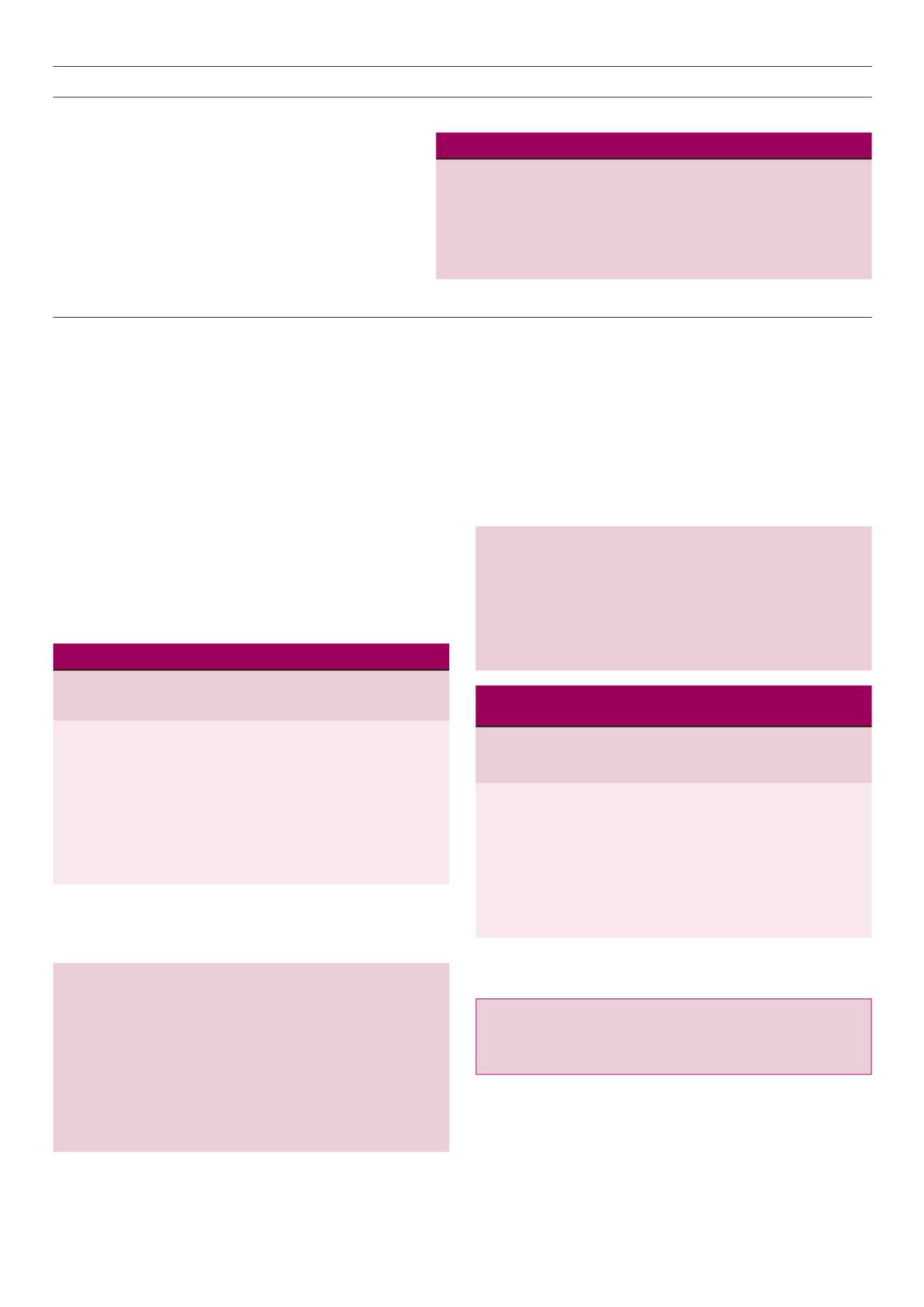
Letter Clinical characteristic
Points awarded
H
Hypertension
1
A
Abnormal renal and liver function (1 point each)
1 or 2
S
Stroke
1
B
Bleeding
1
L
Labile INRs
1
E
Elderly (e.g. age > 65 years)
1
D
Drugs or alcohol (1 point each)
1 or 2
Maximum 9 points
Key learnings
• Kidney disease in the T2DM patient may arise from both hyperglycaemia and
hypertension, and significantly increases mortality and cardiovascular risk
• Diabetes predisposes toward the development of AF, with comorbidity substantially
increasing all-cause mortality and major cardiovascular events
• Risk for development of AF is further increased in the diabetic patient with CKD
• Use of NOACs in diabetic patients with AF is associated with risk reduction for end-
stage renal disease and slower progression to AKI.
world setting, NVAF patients with T2DM were treated with
warfarin or rivaroxaban at reduced doses, as suggested for
the level of renal dysfunction in the patient with comorbid
kidney disease – 24% of patients received a rivaroxaban dose
of 15mg. Consistent with RCT data, there were no changes
in bleeding rates. Observational reports suggest a reduction
in MALE, another signal implying benefit of rivaroxaban
beyond simply the heart, but also for the kidneys and limbs in
T2DM patients with AF.
Among the NOACs we have the choice between one of two anti-
factor Xa inhibitors (rivaroxaban and apixaban) and a thrombin
antagonist (dabigatran). Although there were slight variations in the
Rivaroxaban
Anti-factor Xa
Apixaban
Dabigatran
Antithrombin
}
CHA
2
DS
2
-VASc score
Only males < 65 years can achieve a CHA
2
DS
2
-VASc score < 1
HAS-BLED score
The HAS-BLED score estimates bleeding risk, but except in patients
who have a marginal indication for anticoagulation, the bleeding
risk never outweighs the need to anticoagulate.
Which NOAC?