

















 37 / 42
37 / 42

VOLUME 17 NUMBER 1 • JULY 2020
35
SA JOURNAL OF DIABETES & VASCULAR DISEASE
CASE REPORT
on either rivaroxaban or warfarin. Diabetic patients likely to be at
higher risk showed renal protection using rivaroxaban treatment
compared to warfarin (Fig. 8).
10
It is important to recognise that the microvascular complications
(nephropathy, neuropathy, retinopathy) and the macrovascular
complications (coronary disease, peripheral disease, stroke) are all
manifestations of the same pathobiology of vascular dysfunction,
atherothrombosis and atherosclerosis in the patient with diabetes.
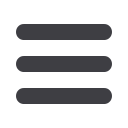
Patients with diabetes and renal impairment have
increased cardiovascular risk
Meta-analysis of 1.2 million people from the Alberta Kidney
Disease Network (AKDN) database and the National Health and
Nutrition Examination Survey (NHANES) 2003–2006 showed, over
a 48-month follow-up, a stepwise increase of cardiovascular risk
in patients with diabetes and CKD as opposed to the presence of
kidney dysfunction only or diabetes only (Fig. 9).
11
Fig. 9.
Patients with diabetes and renal impairment have increased
cardiovascular risk.
11
What is the prevalence of diabetes in randomised
controlled trials of NOAC use in patients with NVAF?
When interpreting the cardiovascular outcomes of randomised
controlled trials (RCTs), it is important to consider the numbers
of diabetic patients participating in these studies. ROCKET AF, in
which almost 40% of patients had T2DM, is very representative of
today’s medical practice (Table 1).
12
Table 1.
Clinical features and prevalence of diabetes in NOAC RCTs of
patients with NVAF
12
Study
RE-LY ROCKET AF ARISTOTLE ENGAGE-AF
Drug
Dabigatran Rivaroxaban Apixaban Edoxaban
Age >75 years
40.1% 43.7% 31.2% 40.5%
CHADS
2
mean
2.2
3.48
2.1
2.8
Previous TIA/
stroke
20.3% 54.9% 19.2% 28.1%
Hypertension
78.9% 90.3% 87.3% 93.7%
Diabetes
23.3%
39.9% 25.0% 93.7%
Heart failure
31.8% 62.6% 35.5% 58.2%
Effectiveness of rivaroxaban in patients with NVAF
and diabetes has been evaluated in RCT and real-
world settings
It is important to be aware that real-world data are consistent
with the results of ROCKET AF. Rivaroxaban, as compared to
warfarin, shows benefit for stroke/ systemic embolism, major
bleeding and intracranial haemorrhage in the diabetic patient
with NVAF (Fig. 10).
Fig. 10.
Rivaroxaban vs warfarin in the diabetic patient with NVAF – RCT and
real-world data.
AF: atrial
fibrillation; NOAC: non-vitamin K antagonist oral anticoagulant; RCT:
randomised controlled trial; TIA: transient ischaemic attack.
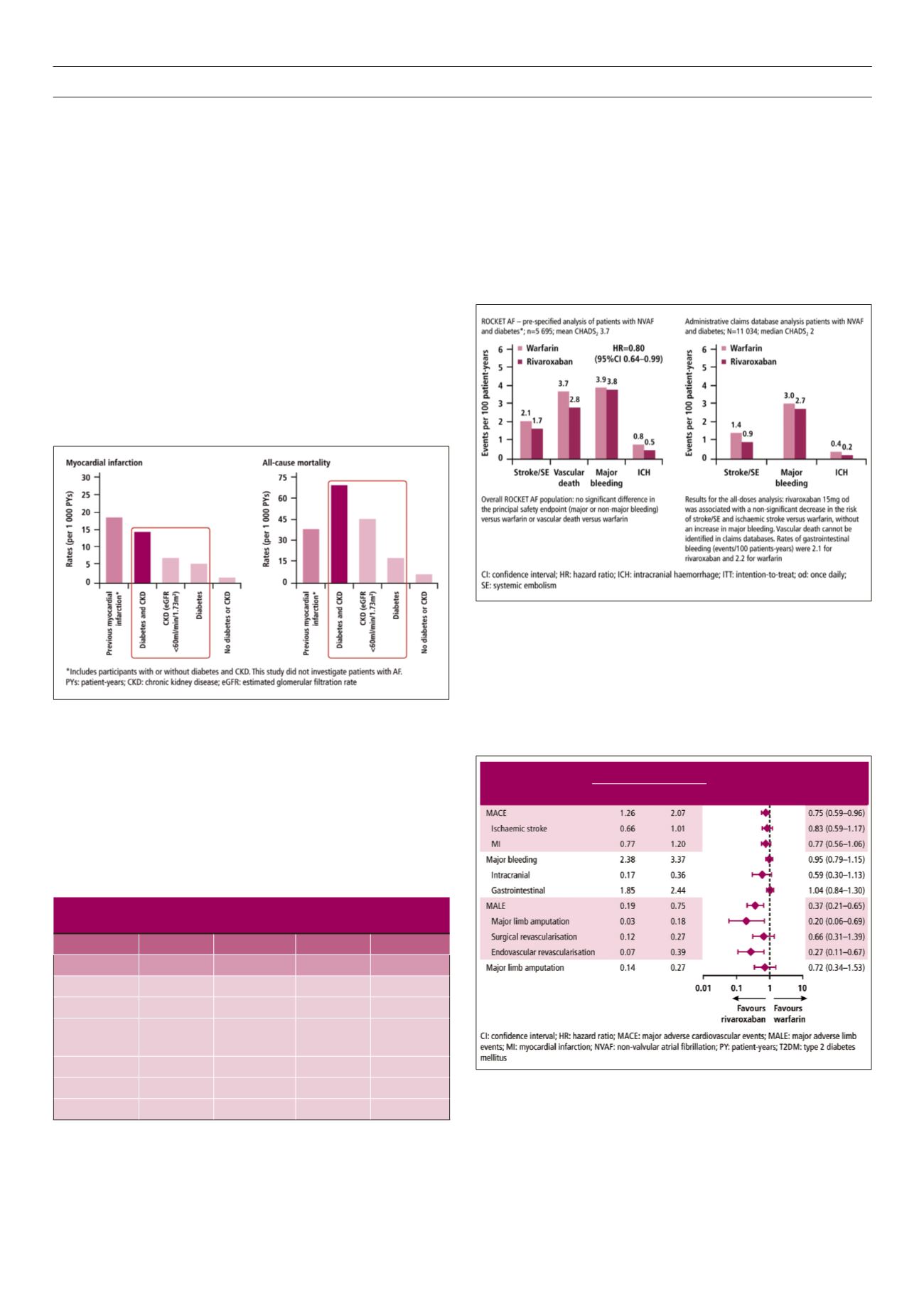
Furthermore, rivaroxaban has been associated with lower risks
of major adverse cardiovascular events (MACE) and major adverse
limb events (MALE) compared to warfarin in patients with NVAF
and T2DM (Fig. 11).
13
MarketScan data also show that in the real-
Fig. 11.
Rivaroxaban was associated with a lower risk of MACE and MALE than
warfarin in patients with NVAF and T2DM.
13
Analysis of
US MarketScan claims data for patients with NVAF and co-morbid
T2DM initiating therapy with warfarin (
n
= 13 946) or rivaroxaban (
n
= 10 700;
24.1% of these received a reduced dose).
Event rate (per 100 PY)
Rivaroxaban Warfarin
HR (95% CI) HR (95% CI)